Case 1
HPI:
36 year-old female with no significant medical history who presents after referral for voice hoarseness. According to the patient, she underwent a C-section 3 months ago (at an outside hospital) complicated by bleeding requiring a second operation (L salpingoophorectomy); however, neither procedure required emergent intubation. She reports that she had some vomiting associated with anesthesia which ultimately required intubation and admission to the MICU for 5-6d. She was discharged 10 days after the initial operation, and both she and her baby were in good health. Two weeks after discharge, she began experiencing throat irritation and 1 month after discharge she noticed voice hoarseness which has been persistent. Today, she denies difficulty swallowing or breathing, F/C, N/V, abdominal pain.
PMH:
None
PSH:
Cesarean x2, L salpingoophorectomy
FH:
Non-contributory
SHx:
Lives at home taking care of 3 children, denies t/e/d
Meds:
None
Allergies:
NKDA
Physical Exam:
| Gen: | WA, NAD |
| Head: | NC/AT |
| OC: | MMM, no lesions, no pharyngeal erythema/exudates, hoarse voice |
| Ears: | EAC clear, TMI b/l |
| Flex: | Posterior commissure edema, cobblestoning, b/l TVC with shiny white masses |
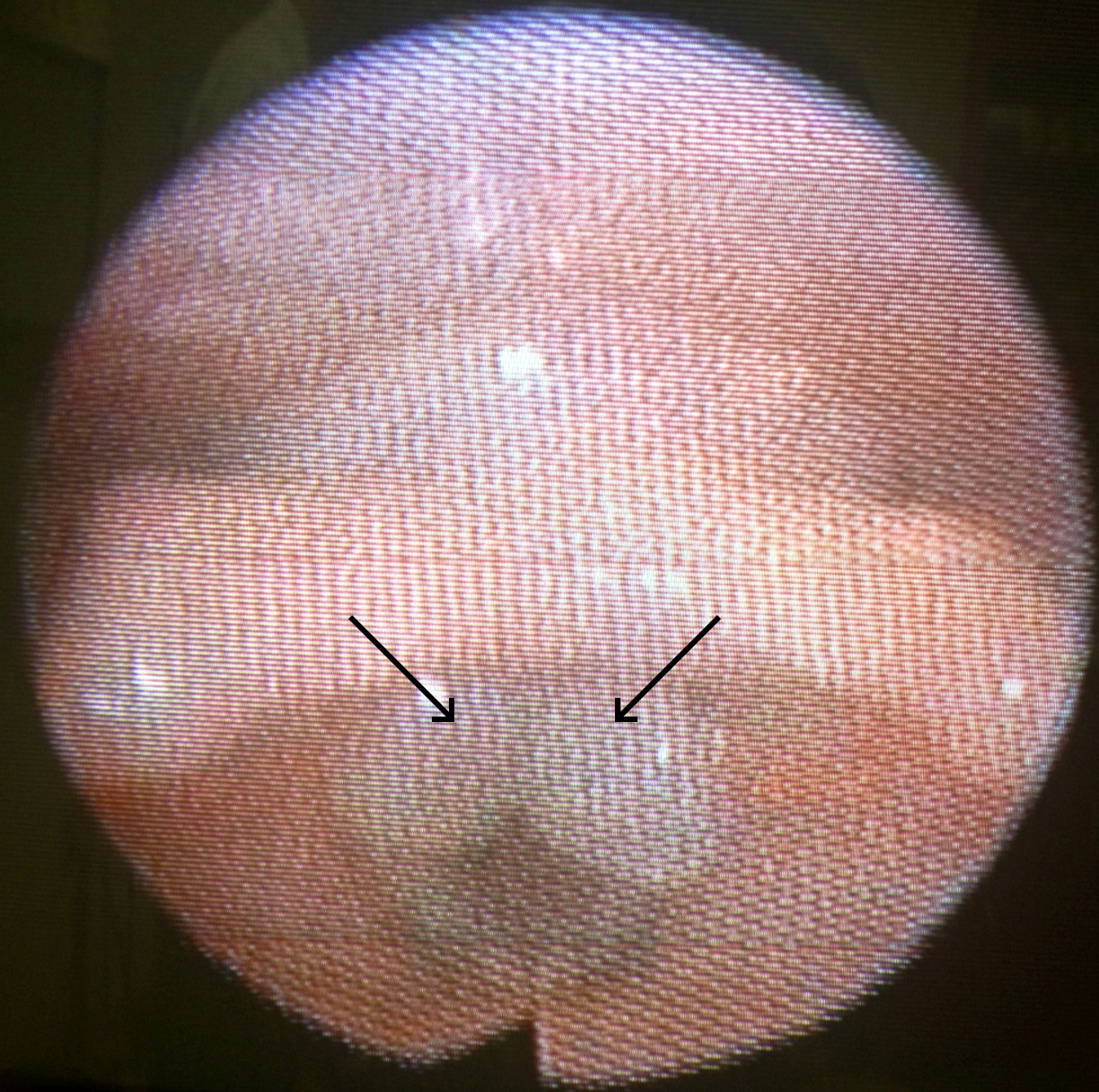
Flexible nasolaryngoscopy image showing trauma granulomata.
Assessment/Plan:
36F, no significant PMH, recent Cesarean and L salpingoophorectomy c/b likely aspiration requiring intubation and mechanical ventilation for several days with onset of progressive voice hoarseness 1mo later. History and flexible nasolaryngoscopy consistent with trauma granulomata, as well as laryngopharyngeal reflux.
- Discussed treatment options with patient, recommend voice rest x2mo and continued monitoring
- Laryngopharyngeal reflux, given dietary/lifestyle education, start omeprazole 20mg p.o. b.i.d.
- RTC 1mo
Case 2
HPI:
51 year-old female with a history of Hepatitis C, COPD and an 80 pack-year smoking history presents with concern about progressive voice hoarseness x2mo. She reports quitting smoking two months ago and is not sure if the hoarseness preceded or followed quitting. She has occasional throat discomfort which is mild. She otherwise denies difficulty or pain with swallowing, worsening shortness of breath, unintentional weight loss.
She also reports a new mass on her neck which she first noticed yesterday. Denies associated pain, or surrounding skin changes.
PMH:
- Hepatitis C
- COPD
PSH:
- Hysterectomy
FH:
Non-contributory
SHx:
80 pack-year smoking history, no current EtOH, drug use (previously used heroin and opiates)
Meds:
- Methadone
- Elavil
- Multiple unknown inhaled medications
Allergies:
- Naproxen (swelling)
Physical Exam:
| Gen: | WA, NAD |
| Head: | NC/AT |
| Eyes: | PERRL, EOMI |
| Ears: | b/l EAC erythema, TMI, no lesions/exudates |
| OC: | MMM, no lesions |
| Neck: | Supple, no thyroid enlargement, no cervical lymphadenopathy, 5x6cm soft, round, mobile, non-tender mass on left lateral neck w/o overlying skin changes |
| Flex: | Diffuse laryngeal damage, thickened posterior commissure, right TVC with area of leukoplakia, left TVC appears irregular |
Assessment/Plan:
51F hx HepC, COPD, 80py smoking, presenting with voice hoarseness x2mo. History concerning for malignancy, exam today shows significant laryngeal damage and vocal cord irregularities warranting further evaluation. Possible component of fungal infection 2/2 inhaled steroid use for COPD, plan to reduce potentially aggravating factors (treat fungal infection, voice rest) and repeat evaluation. Neck mass possibly lipoma however will evaluate further given concern for malignancy.
- Start fluconazole 100mg two tables p.o. on day1, 100mg p.o. daily x7d
- Start nystatin 100,000 units/mL 10mL gargle and swallow t.i.d. x2wks
- Advised voice rest
- RTC in 3wks
- CT neck/soft tissue w/wo IV contrast to evaluate neck mass
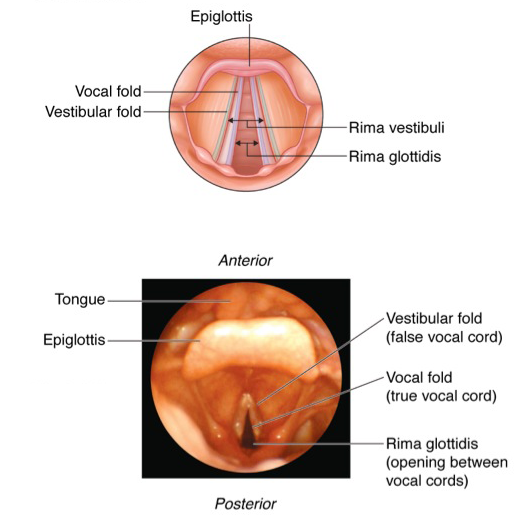
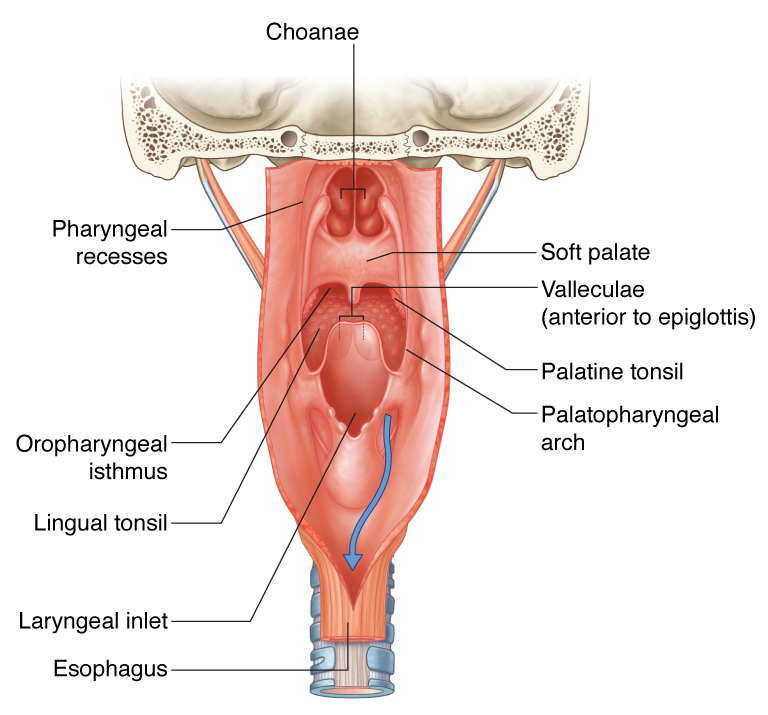
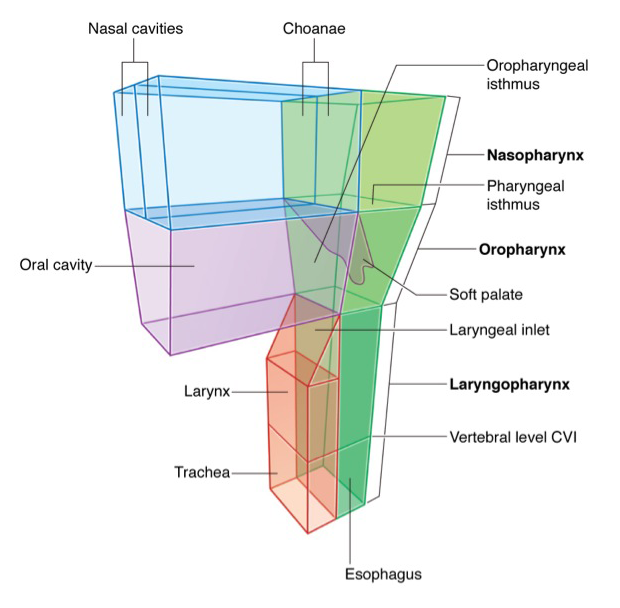
Anatomy of the Pharynx/Larynx:
Physiology of Voice Production: 1
Voice is produced through the passive vibration of vocal folds in an air stream and requires:
- Adequate Air Stream
- Smooth vocal fold edges
- Vocal folds with normal vibratory properties
- Appropriate vocal fold positioning
Differential diagnosis of dysphonia (hoarseness): 1,2,3

Characteristics of Hoarse Voice: 5
| Characteristic | Likely cause |
|---|---|
| Breathy | Vocal cord paralysis |
| Hoarse | Vocal cord lesion, LPR |
| Low-pitched | Reinke’s edema, vocal abuse, LPR |
References:
- Mau, T. (2010). Diagnostic Evaluation and Management of Hoarseness. Medical Clinics of North America, 94(5), 945–960. doi:10.1016/j.mcna.2010.05.010
- Feierabend, R. H., & Shahram, M. N. (2009). Hoarseness in adults. American family physician, 80(4), 363–370.
- Schwartz, S. R., Cohen, S. M., Dailey, S. H., Rosenfeld, R. M., Deutsch, E. S., Gillespie, M. B., Granieri, E., et al. (2009, September). Clinical practice guideline: hoarseness (dysphonia). Otolaryngology. doi:10.1016/j.otohns.2009.06.744
- Bruch, J.W., Kamani D.V. Diaphragmatic pacing. In: UpToDate, Basow, DS (Ed), UpToDate, Waltham, MA, 2013.
- Rosen, C. A., Anderson, D., & Murry, T. (1998). Evaluating hoarseness: keeping your patient’s voice healthy. American family physician, 57(11), 2775–2782.
Pingback: Differential Diagnosis of Dysphagia