Brief HPI
An approximately 40 year-old male with a history of aortic stenosis s/p mechanical aortic valve replacement (on Coumadin) as well as hypertension presented to the emergency department with a chief complaint of severe headache. The patient was in severe distress on arrival and was unable to provide detailed history, he complained of two days of severe left-sided headache while clutching his head and groaning. Examination was notable for sensory localization with directed movements of right hemibody, and no apparent response on the left. He was taken to emergently for CT head non-contrast.
Imaging
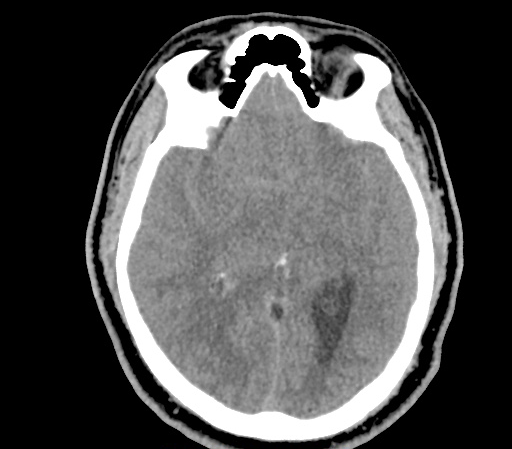

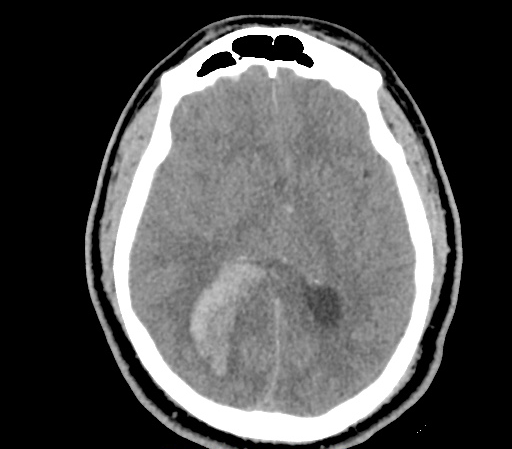
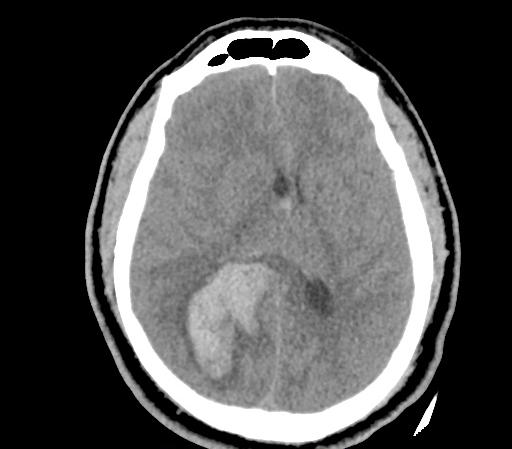
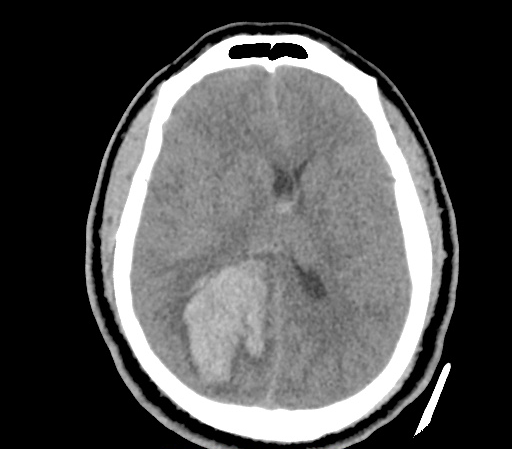
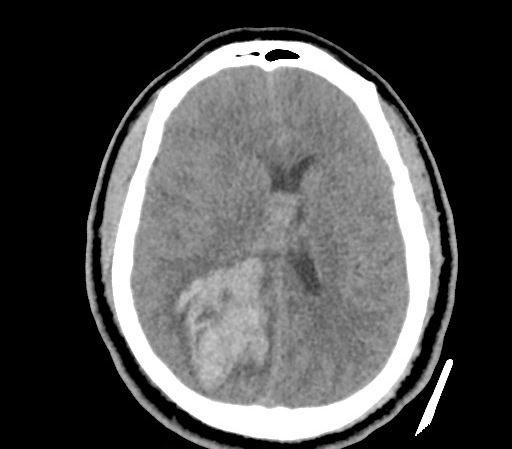
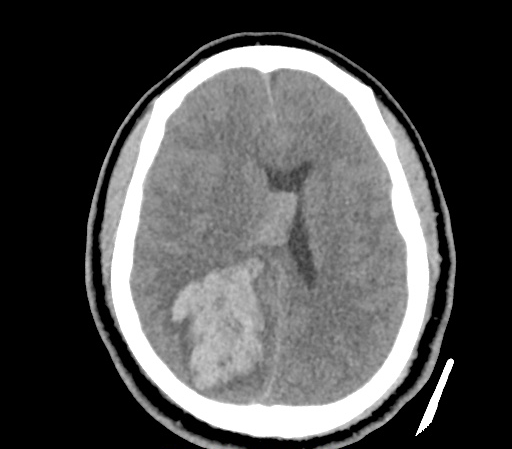





CT Head non-contrast
57 mm right posterior parenchymal hemorrhage with intraventricular component. Moderate edema, mass effect and 9 mm of midline shift.
ED Course
Admission INR was 2.9, the patient received 25 units/kg of PCC as well as vitamin K 10mg IV x1. Neurosurgery was consulted and the patient was taken to the operating room for management.
Management of Supratherapeutic INR and Complications of Anti-Coagulation

References
- Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; (6 Suppl):160s