
Post Category → This Site
A history of the ddxof: mobile application
I’ve wanted a mobile companion application for ddxof for a while. I’m not entirely sure that anyone else feels strongly about it, but I use the content regularly on shift and trying to load even the mobile-optimized website on my phone was cumbersome. Dropbox worked for a while but it didn’t maintain the taxonomy I’d assigned on the website and text content wasn’t included.
While I have some experience with web development, a quick peek at Objective C and native app development suggested I would be in over my head. So, I sought some funding, designed a few basic screens in Sketch, and waited to see what the development team came up with.

Sketches of different screens on the app
Version 1.0

The app hung on this screen for 20 seconds on launch
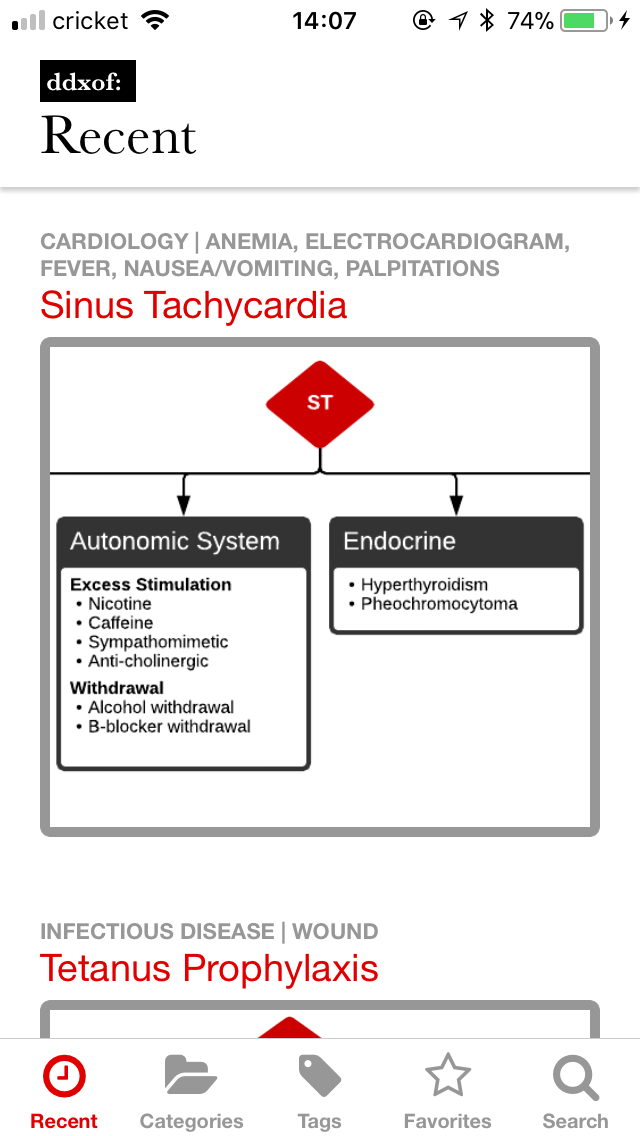
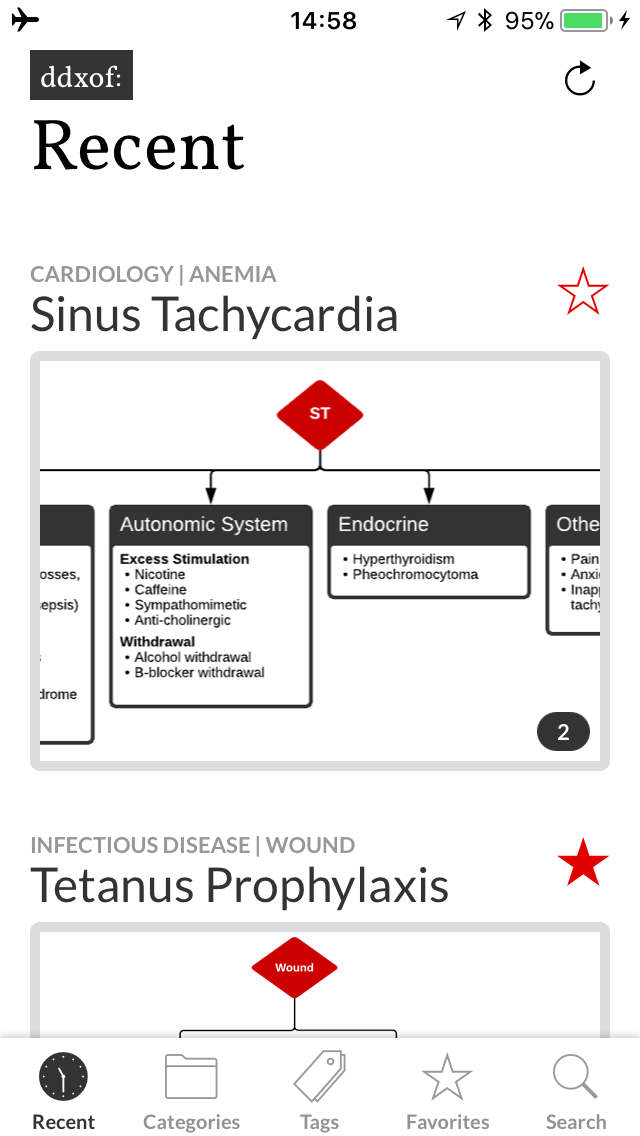
When it loaded, things looked pretty good
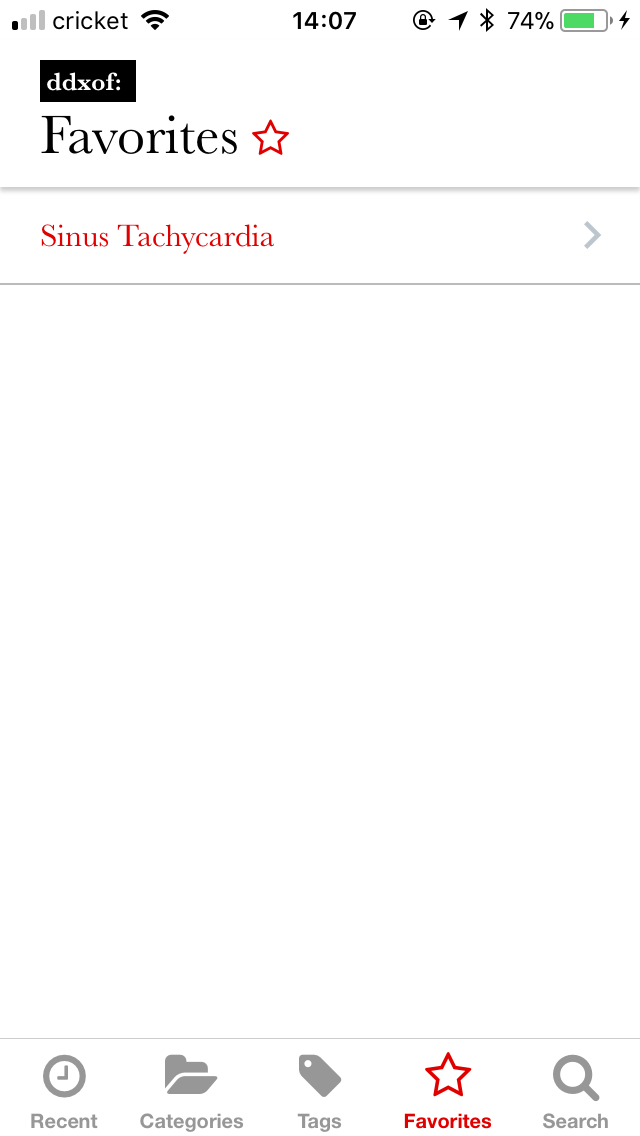
It even had working favorites
In November, I saw the final product and it was a bit of a fixer-upper. Much of the functionality was present (including adding Favorites). Unfortunately, less attention seemed to have been paid to certain usability aspects and the visual style I’d developed in the design compositions.
Most glaring was the lack of any representation of a loading state. It pained me to watch coworkers download the app and see a blank screen that ignored their interaction attempts for a solid 20 seconds on the app’s initial launch.
Luckily, I got access to the source code and found that it was built with something called React Native. As I sifted through the code, I realized that I recognized and (mostly) understood what was happening. It was basically JavaScript, I know JavaScript! The display and styling portions were also easy to grasp as they’re similar to HTML and CSS respectively.
I tried to work backwards from the code I’d received but it was just too hard to grasp. The extent of my JavaScript experience prior to this was rudimentary so after going back and forth a few times between attempting to improve upon the existing app and just starting from scratch, I decided to dive in and begin anew.
Version 2.0
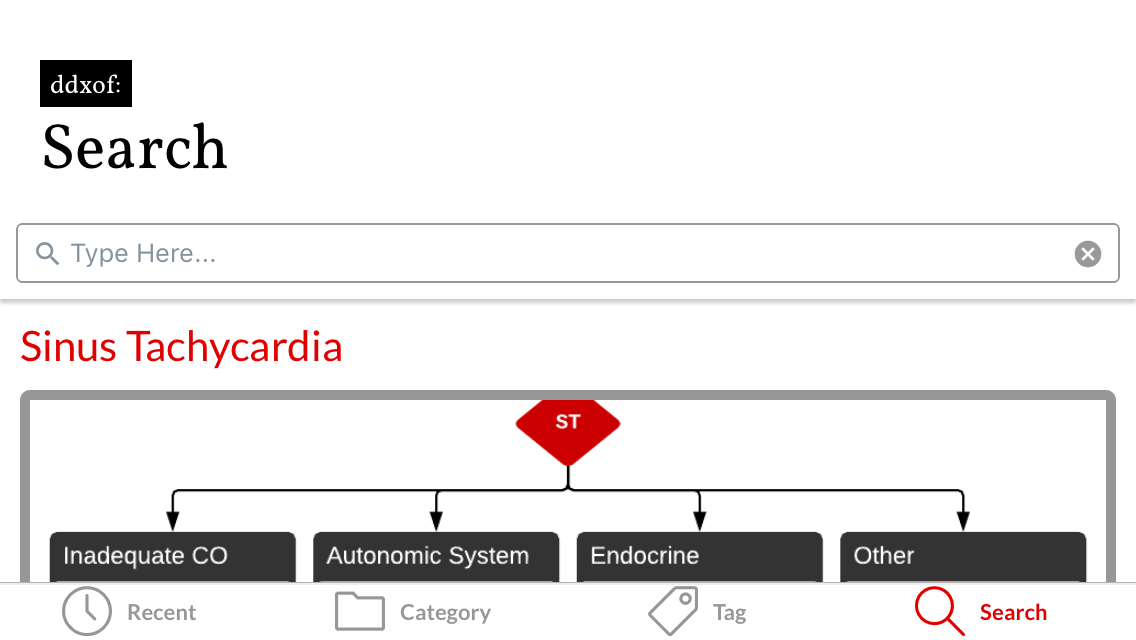
A real loading indicator
I lost a few things, no multiple algorithms, no categories/tags
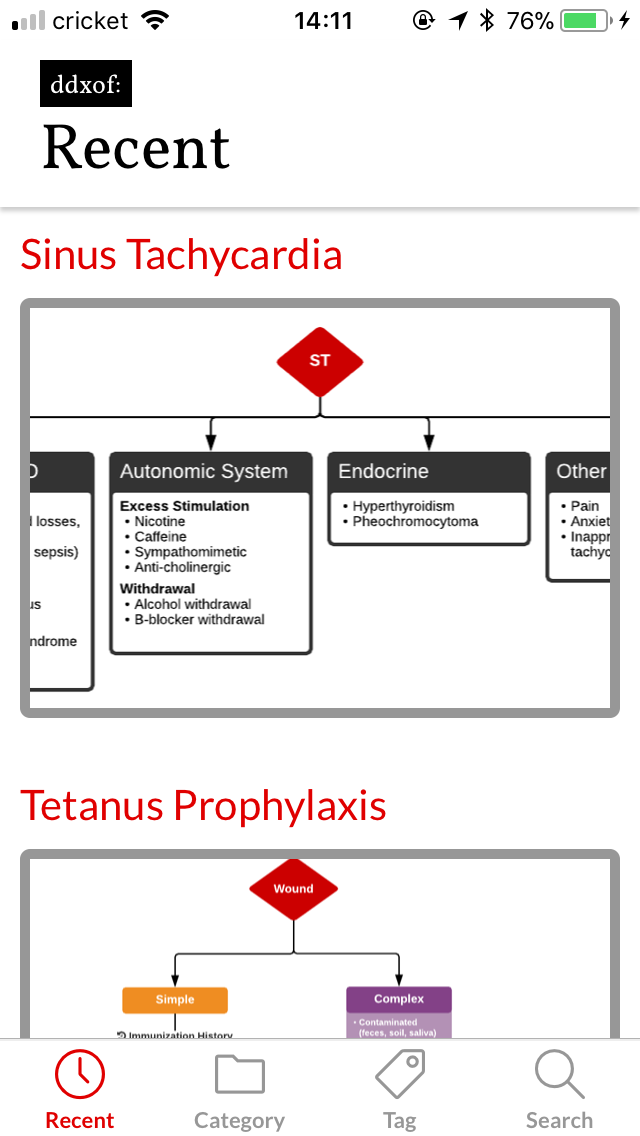
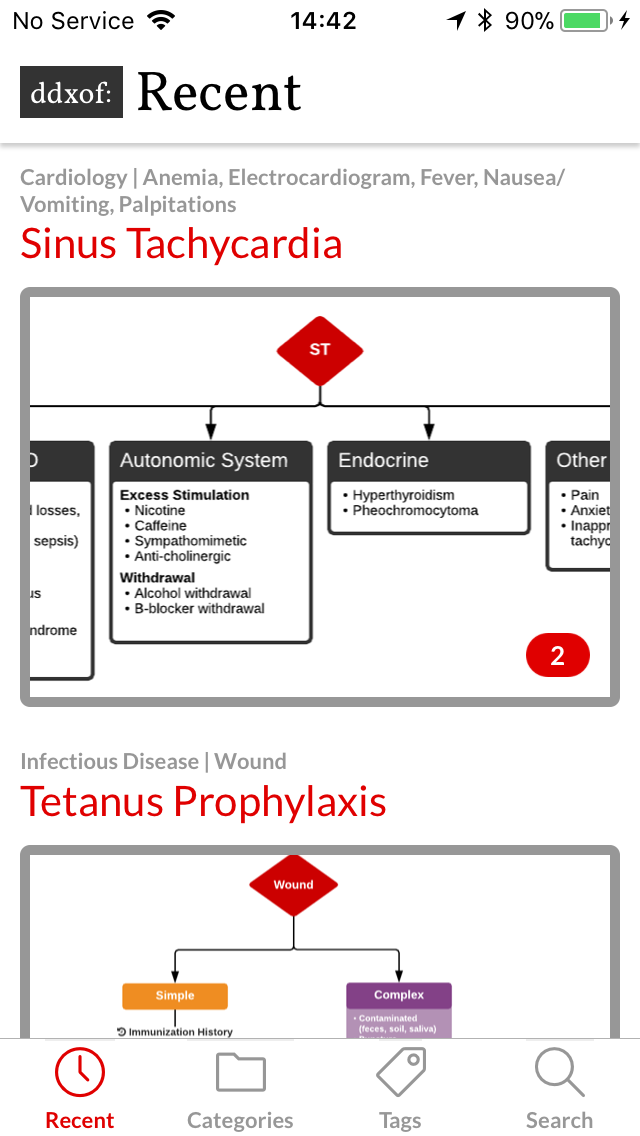
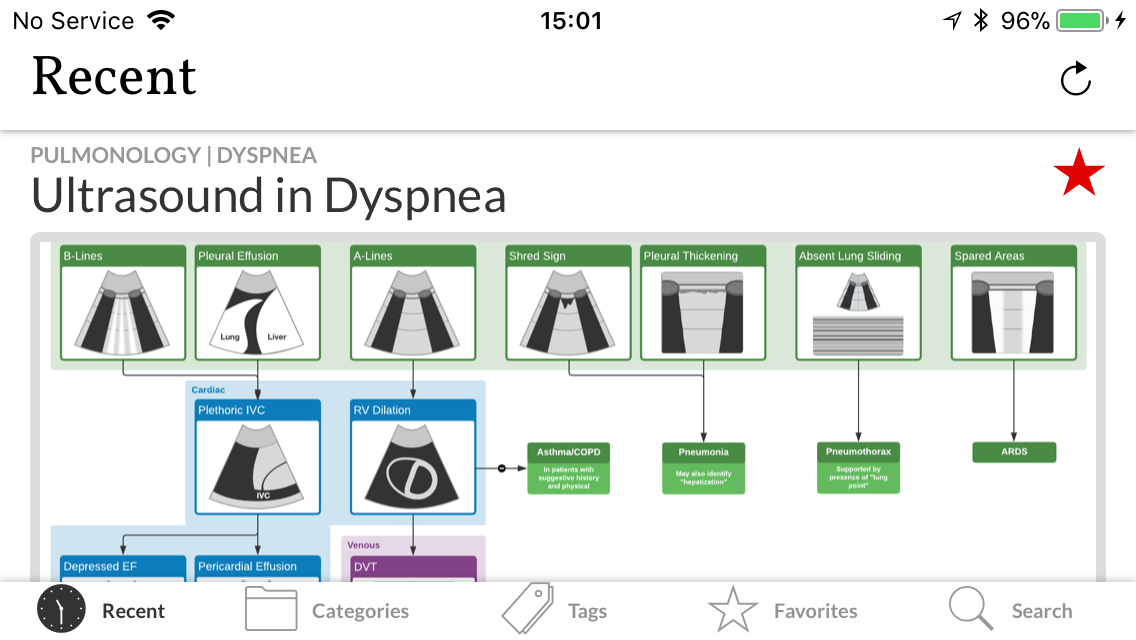
By version 2.3, we had post categories/tags and a gallery view for multiple algorithms
Exactly 1 month later, I released version 2.0 of the ddxof: mobile application. Since it was built from scratch, I had to remove some of the features that were too complex for me to develop. Removing the option to save favorites was a tough choice but I was excited to have a version of the application that at least wouldn’t make me cringe when I saw it in use.
The only reason I was even able to get that far was the truly impressive community surrounding React Native. I thought of them a bit like plugins, and using a few components really simplified the process of interacting with the website’s API and storing content for offline use.
In landscape mode, the header occupied pretty much the entire screen
Version 2.4.2 shrunk the header down
Over the next two months, I worked on iterative functional and visual improvements including better server- and client-side caching, and the ability to see all of post’s algorithms (with an image gallery “plugin”). Things settled down by version 2.4.2, it worked, was mostly bug free, and I took a break.
Version 3.0
As I used the app more, a few things kept bugging me. I really missed being able to save favorites and I was often annoyed that the app didn’t allow interaction during attempts at refreshing content (even though usable cached content was available).
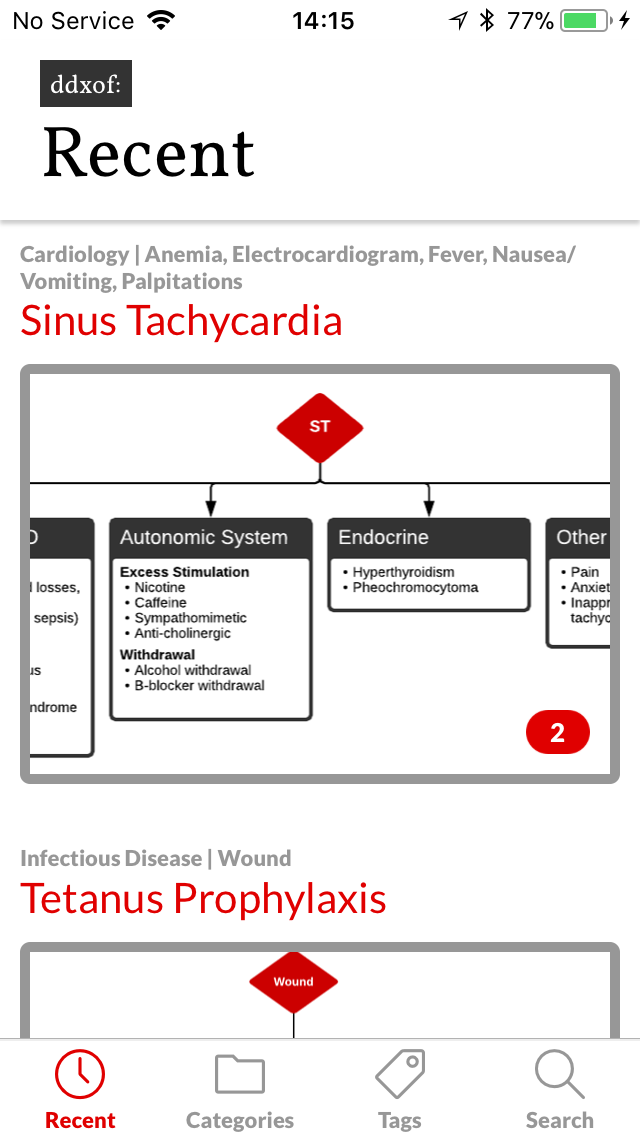
Version 3.0 with a more subdued color scheme
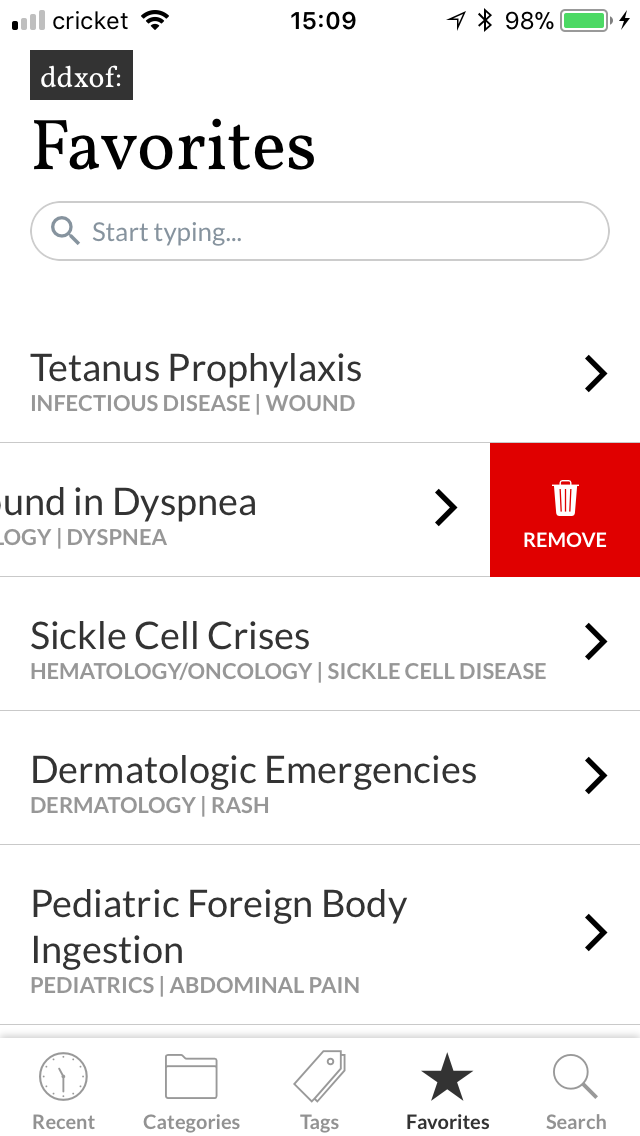
Favorites are back

Cached content remains accessible if a network error occurs
I knew favorites was going to be a problem, I’d tried tackling it earlier when I started working on version 2.0 but had given up. The problem is that an article marked as a favorite needs to be recognized across all parts of the application. This notion of state management in React Native seemed to commonly be handled by a library called Redux. However, despite my best efforts I simply could not wrap my head around the logic. After all, I’m still not a developer and I found myself getting lost in descriptions of “actions” and “reducers”. I was thrilled when I found Mobx which accomplished everything I needed in a much more understandable fashion. My favorites list became an observable that I could access and remained alive wherever I needed it and making the information persist on the user’s device was laughably easy with another plugin.
Using Mobx also meant that I could check for content updates in the background without interrupting the user’s ability to interact with cached content. The small indicator area lets users refresh the content, notify them of a refresh attempt and even connection errors.

The uncollapsed header in landscape mode
The header animates down when scrolling
I also took the opportunity to touch up a few interface issues. The header shrinks with a hopefully-subtle animation when scrolling to provide more space for content. I was also finding the red a bit overwhelming, the muted grays are much more my style.
I’m happy to announce that version 3.0 is now available on the App Store and Google Play Store. Please try it out and let me know what you think!
Mobile Application

A System for Differential Diagnosis
Given the objective of this site – namely to approach the evaluation of patients in a systematic fashion – I thought it would be useful to put some thought into how best to develop these systems. The method I’ll detail below might be cumbersome to apply in every situation, but (at this point at least) it is the best way to ensure that nothing is overlooked.
A System for Differential Diagnosis:

Any illness or abnormality for which a patient could seek medical attention (or a colleague, consultation) can be broadly encompassed by the statement above. The differential diagnosis is developed by delineating the chief concern(s) or primary aberrant signs, and selecting a relevant mixture of disease processes and organ systems. The differential can be narrowed by determining subjective and objective details surrounding the chief concern. The differential can be broadened by expanding each major category into subcategories.
References:
- Benbassat, J., & Bachar-Bassan, E. (1984). A comparison of initial diagnostic hypotheses of medical students and internists. Journal of medical education, 59(12), 951–956.
- Bowen, J. L. (2006). Educational strategies to promote clinical diagnostic reasoning. The New England journal of medicine, 355(21), 2217–2225. doi:10.1056/NEJMra054782
- Coderre, S., Mandin, H., Harasym, P. H., & Fick, G. H. (2003). Diagnostic reasoning strategies and diagnostic success. Medical education, 37(8), 695–703.
- Fulop, M. (1985). Teaching differential diagnosis to beginning clinical students. The American journal of medicine, 79(6), 745–749.
- Graber, M. L., Tompkins, D., & Holland, J. J. (2009). Resources medical students use to derive a differential diagnosis. Medical teacher, 31(6), 522–527.
- Sapira, J. D. (1981). Diagnostic strategies. Southern medical journal, 74(5), 582–584.
Intro to ddxof
I’m a medical student currently rotating through clinical clerkships resident assistant professor in emergency medicine. The purpose of this website is to force me to learn. Recently, I’ve found it increasingly difficult to study from review books, and even more difficult to recall and apply that information practically. What has been working is reading heavily about specific cases I’ve seen. Having a real person in mind, hearing their complaints, doing their examination and then supplementing the experience with targeted reading sticks far better.
As for the format, something that has been hammered into me over the past year is to be systematic in everything I do. The benefits being that I’m less likely to miss stuff if I approach everything the same way. The other benefit for me is that I find these systems to be a better way to learn. Less mnemonics, more flowcharts.
So, I’ll select appropriate cases I encounter (altering identifying information of course), read into it a bit, and create a systematic approach for the evaluation, diagnosis and management of that chief complaint.
The site’s going to be a bit rough, the goal is to make it easy to quickly archive these experiences for future reference and learning.