As with the systematic approach preferred for the evaluation and management of other processes explored on this site, a similarly structured method for the interpretation of imaging commonly obtained in the emergency department may afford the same benefits – namely, the timely identification of pathology while avoiding costly missed diagnoses. In this post, I propose an approach to the interpretation of computed tomography of the abdomen and pelvis.
Aorta Down
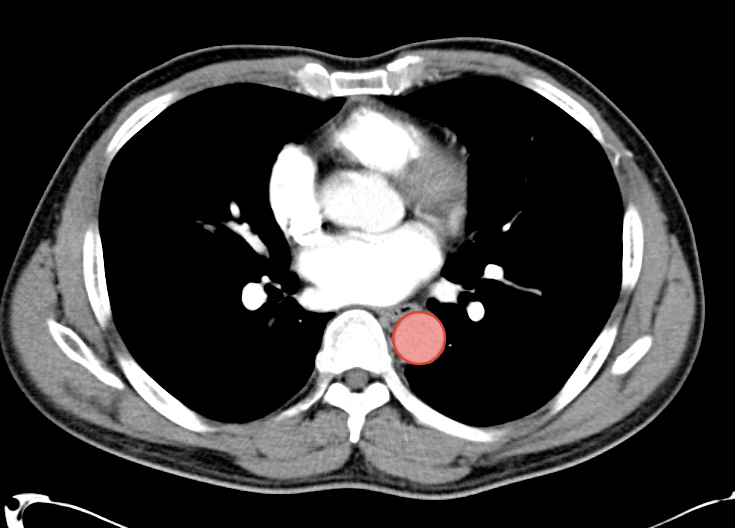
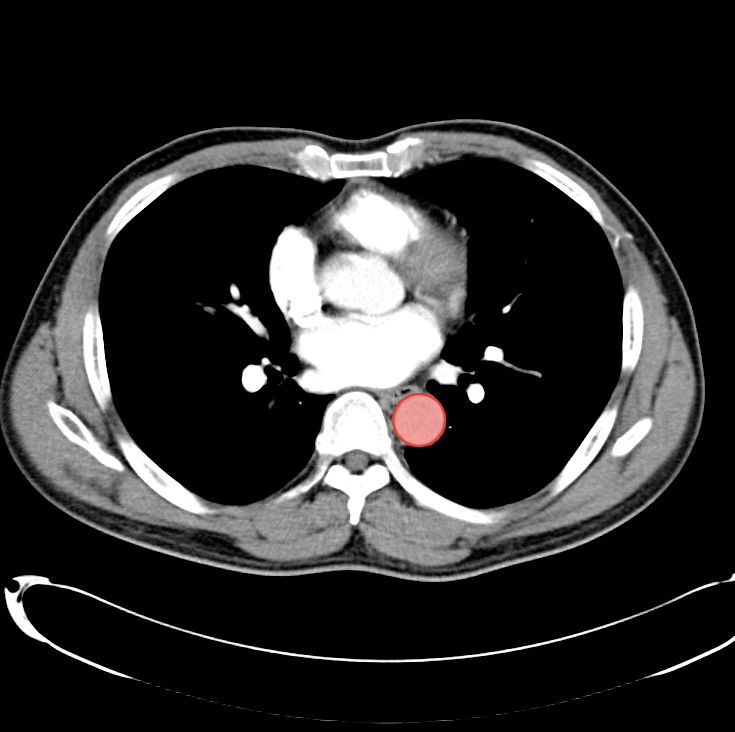
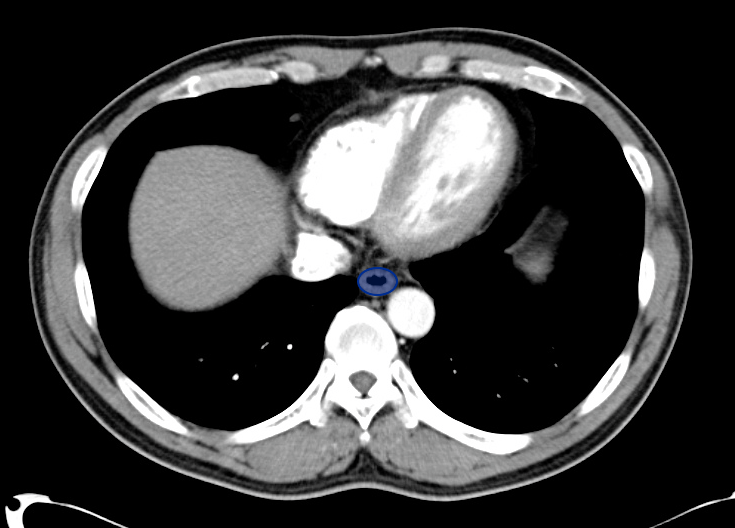
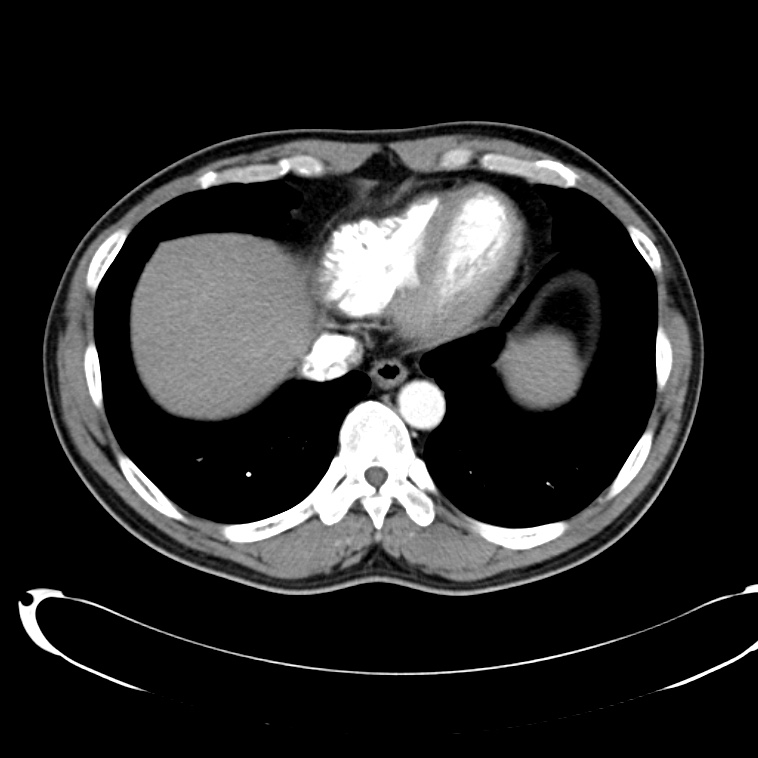
Thoracic Aorta
Start with the descending thoracic aorta
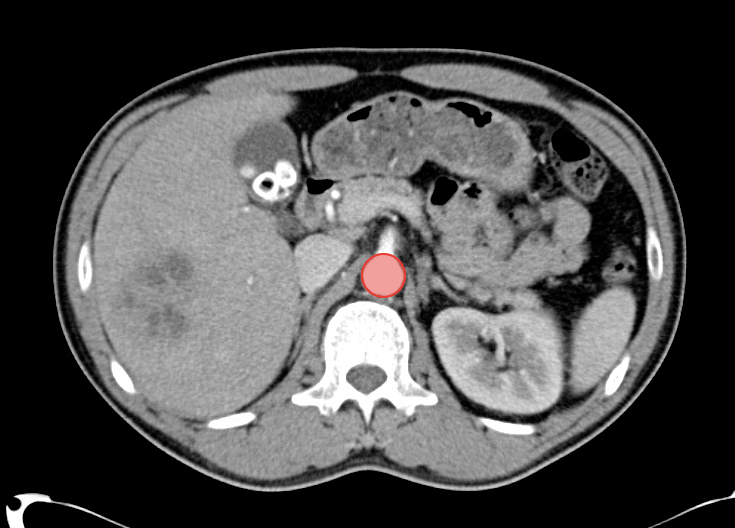
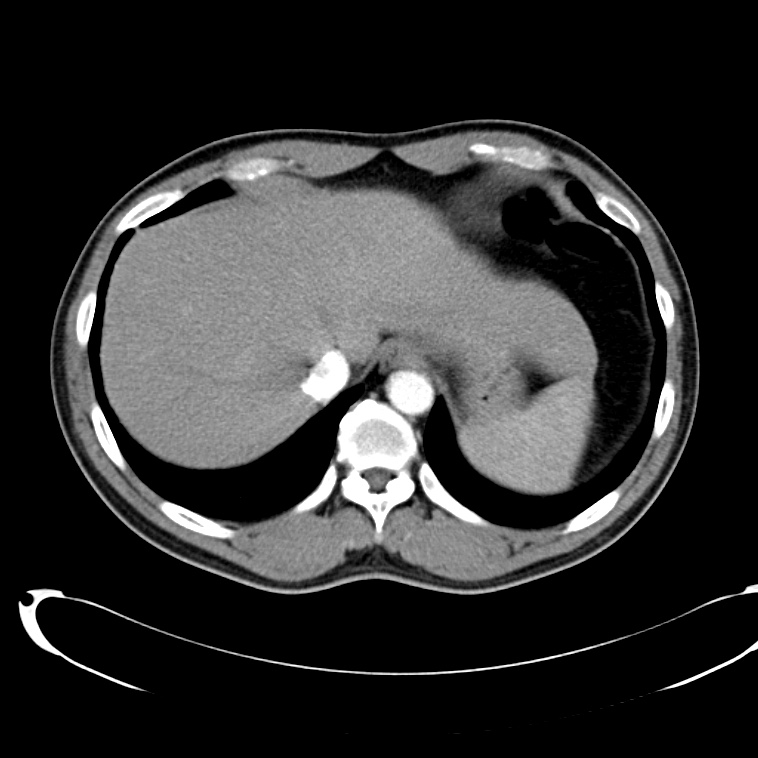
Abdominal Aorta
Follow the abdominal aorta down including its branches (celiac, SMA, paired renal arteries, IMA)
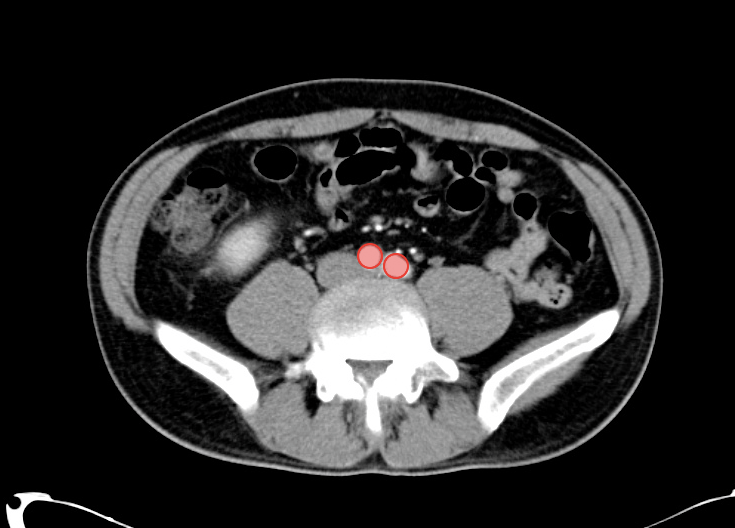
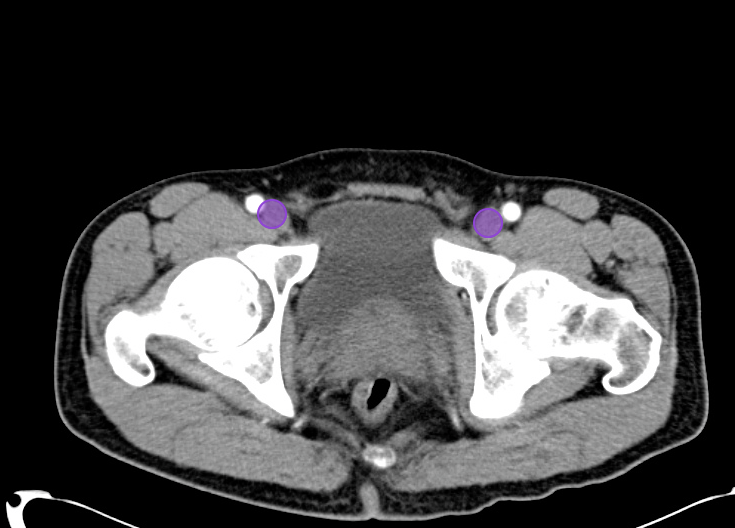
Aortic Bifurcation
Continue to the bifurcation of the abdominal aorta to the left and right common iliac arteries
Veins Up
Femoral Veins
Start with the left and right femoral veins
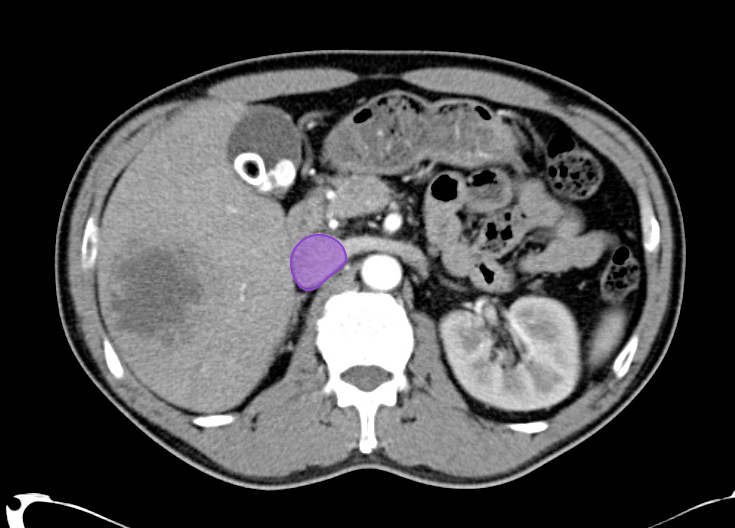
Inferior Vena Cava
Follow the inferior vena cava up
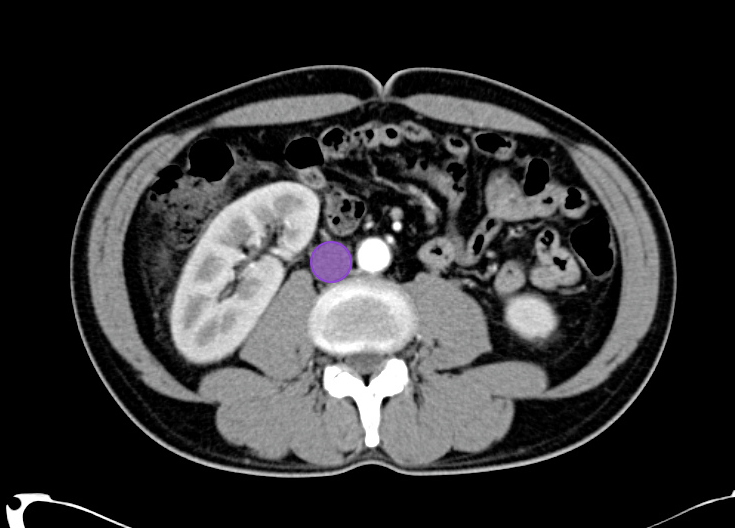
Infrahepatic IVC
The inferior vena cava gains contrast from the renal veins
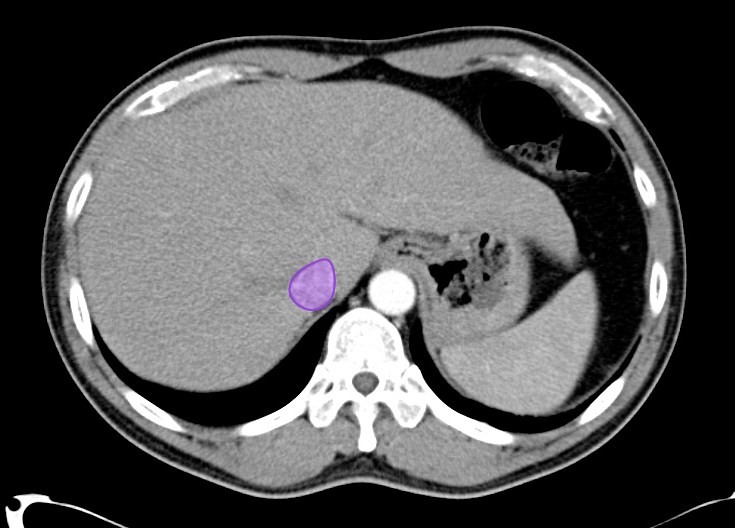
Right Atrium
The inferior vena cava empties into the right atrium
Solid Organs Down
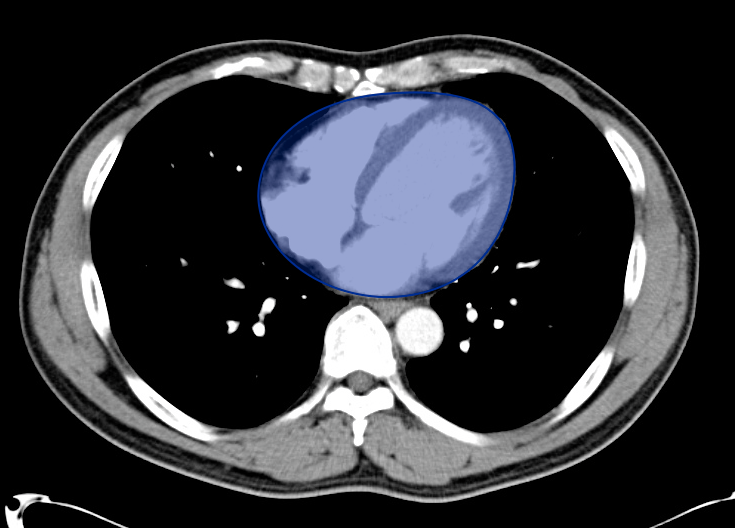
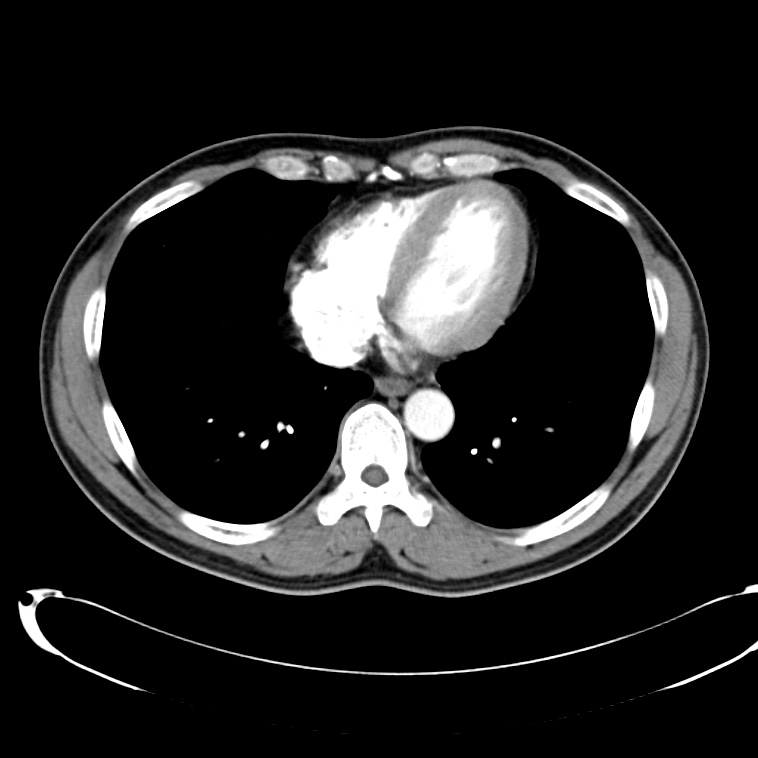
Heart and Pericardium
Evaluate for the presence of a pericardial effusion or cardiomegaly
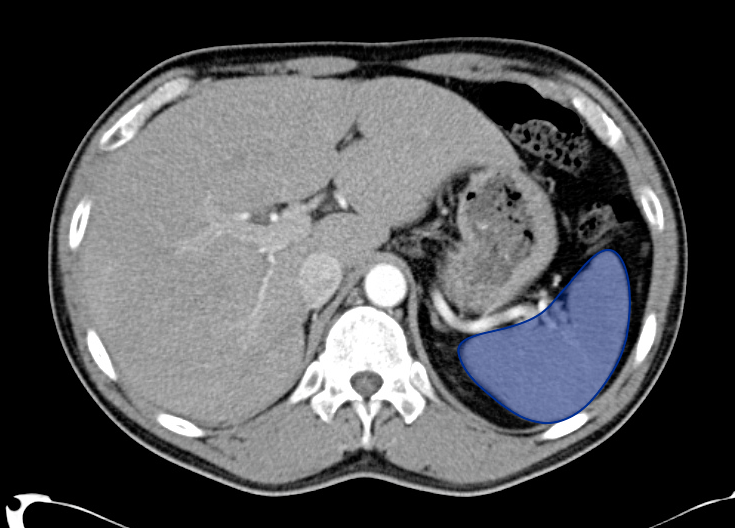
Spleen
Heterogenous contrast-enhancement is normal
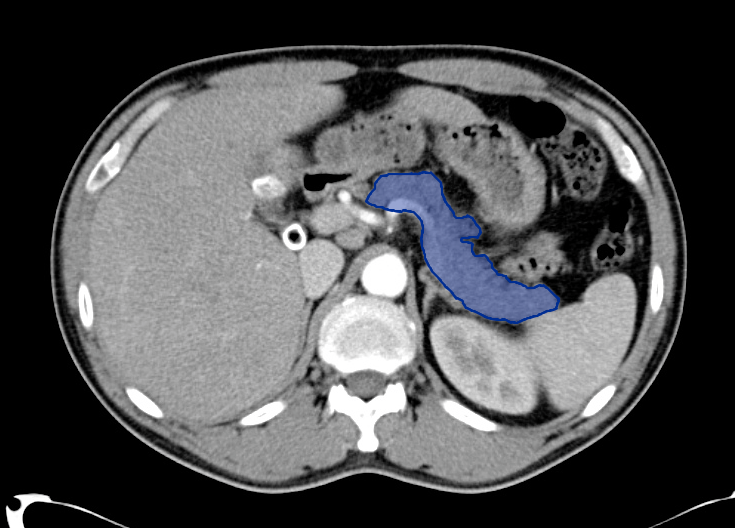
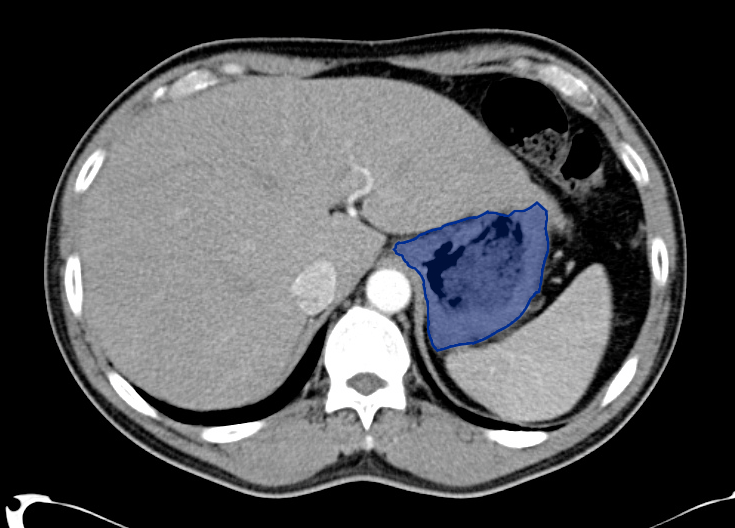
Pancreas
The tail of the pancreas lies in the hilum of the spleen
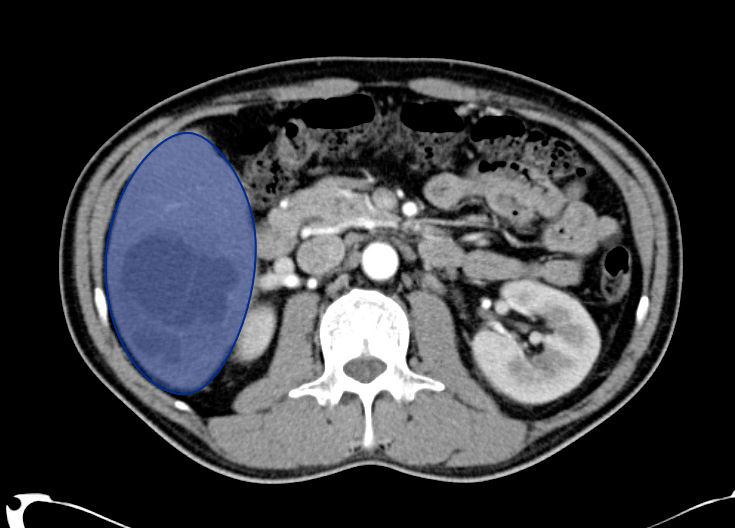
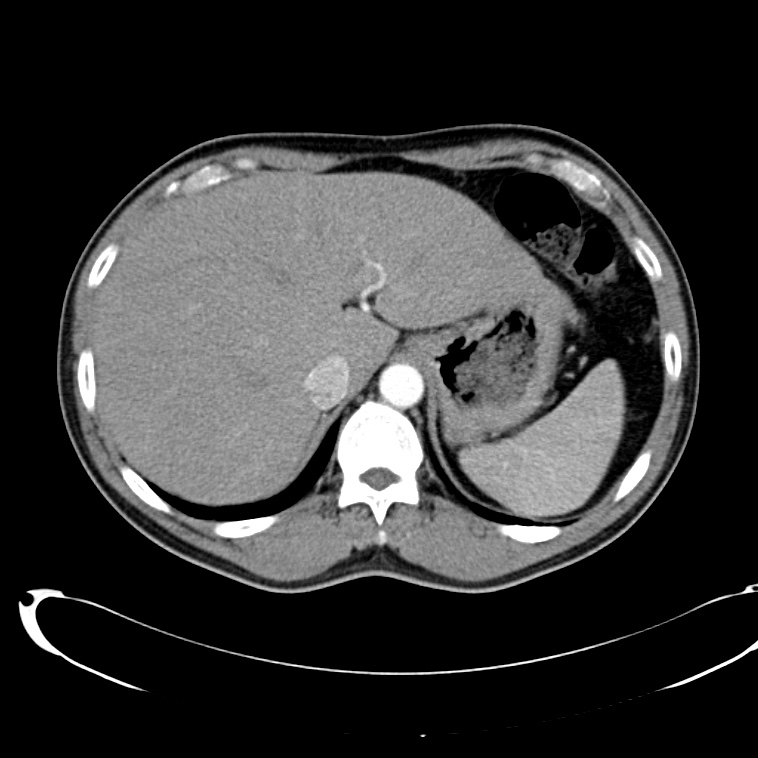
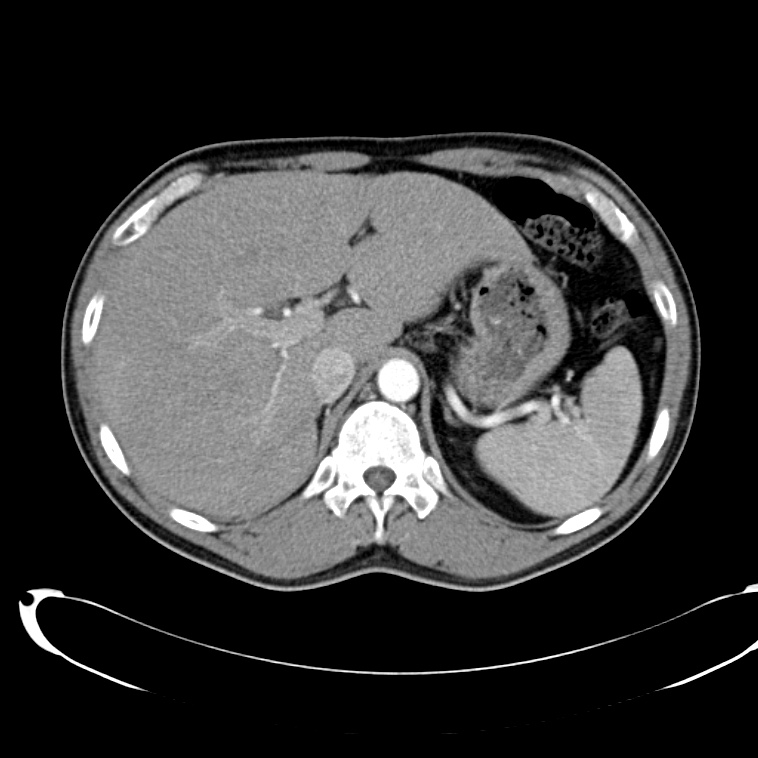
Liver
Evaluate the intrahepatic bile ducts for dilation or pneumobilia, portal venous system for gas, and liver parenchyma for vascular abnormalities or abscesses

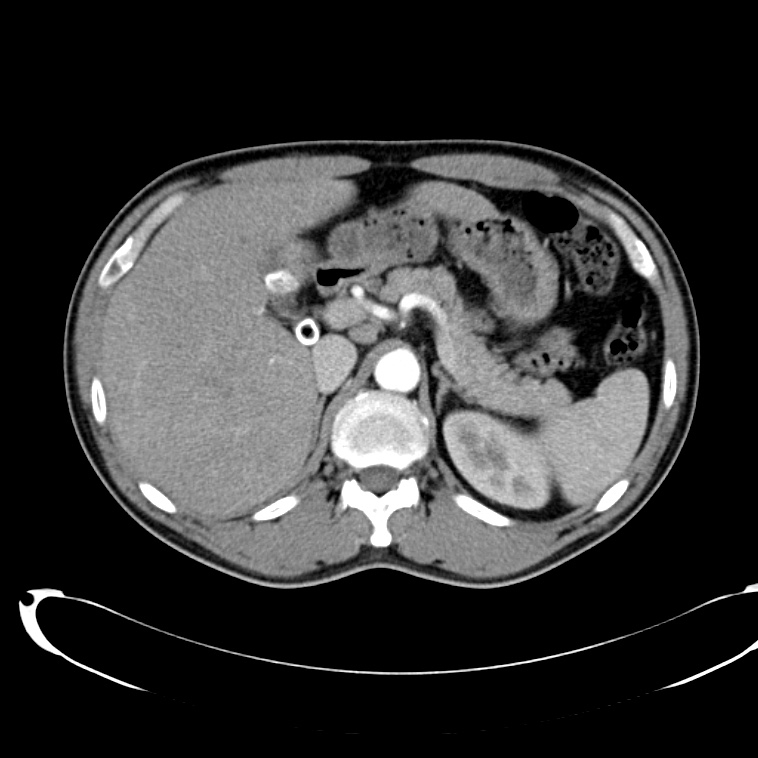
Gallbladder
Evaluate for radioopaque stones, pericholecystic fluid or surrounding fat stranding
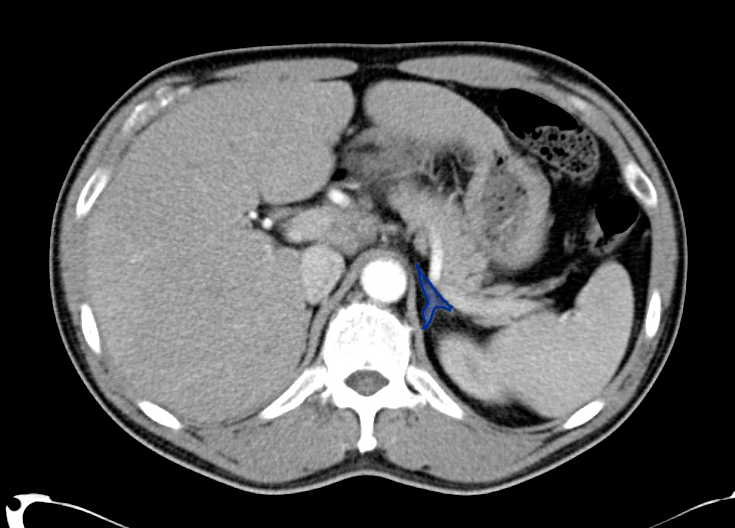
Adrenal
A wishbone-shaped structure superior to the kidneys
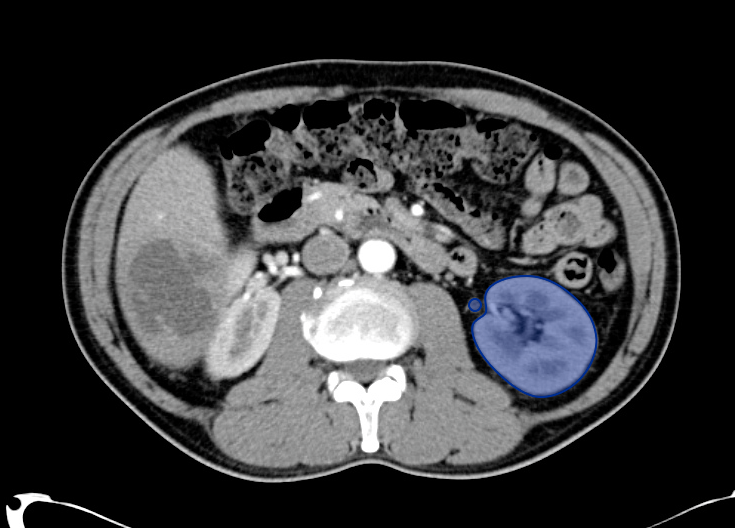
Kidney and Ureter
Evaluate for hydronephrosis or hydroureter

Bladder
Continue down into the pelvis; in a female patient the evaluation should include the uterus and adnexa
Rectum Up

Rectum
Having reached the inferior-most portion of the image following solid organs, move upward again from the rectum
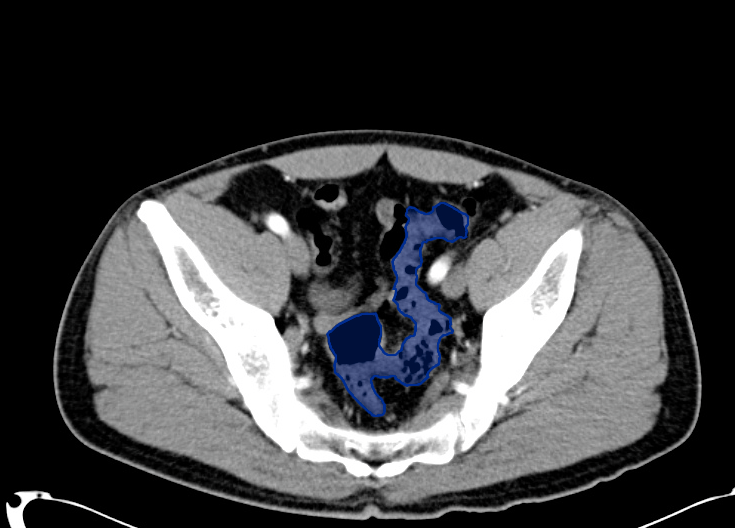
Sigmoid
Evaluate the sigmoid colon for diverticulitis

Transverse
Continue following the sigmoid colon up the descending colon to the transverse colon and the hepatic flexure
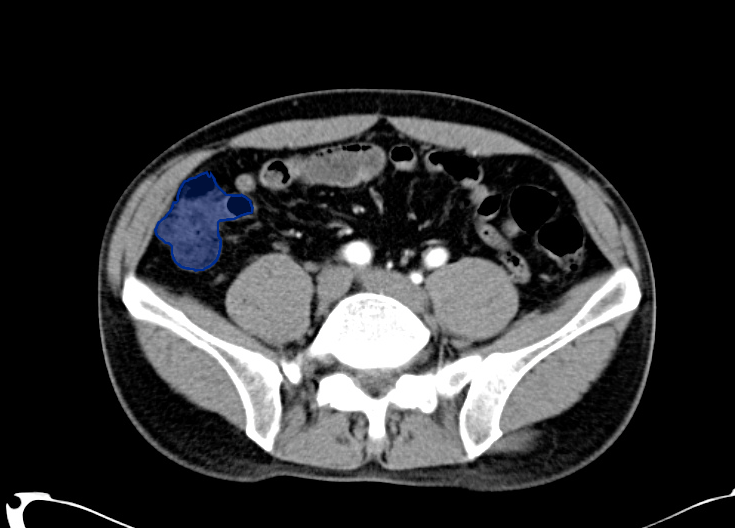
Cecum
Continue down the ascending colon to the cecum

Appendix
At the cecum, attempt to identify a small tubular structure (the appendix) - evaluate for periappendiceal fat stranding, perforation or abscess
Esophagus Down
Esophagus
Start at the esophagus, evaluate for perforation or hernia
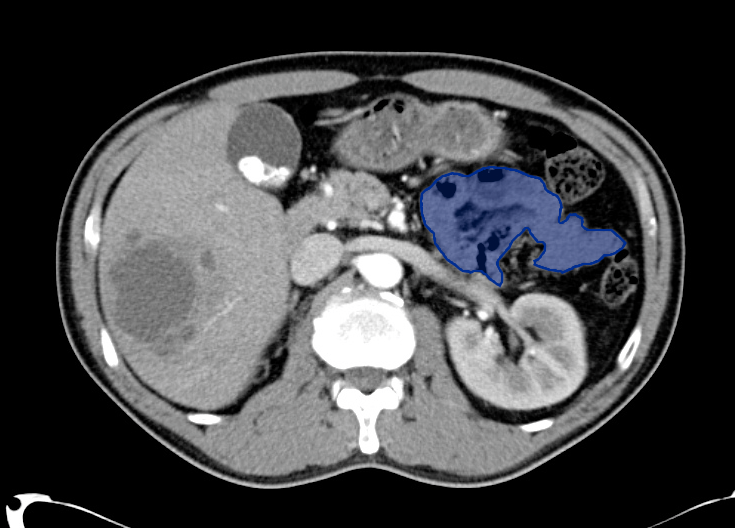
Stomach
Continue to the stomach and duodenum
Small Bowel
Evaluate the small bowel for obstruction (dilation, air-fluid levels)
Tissue-specific Windows
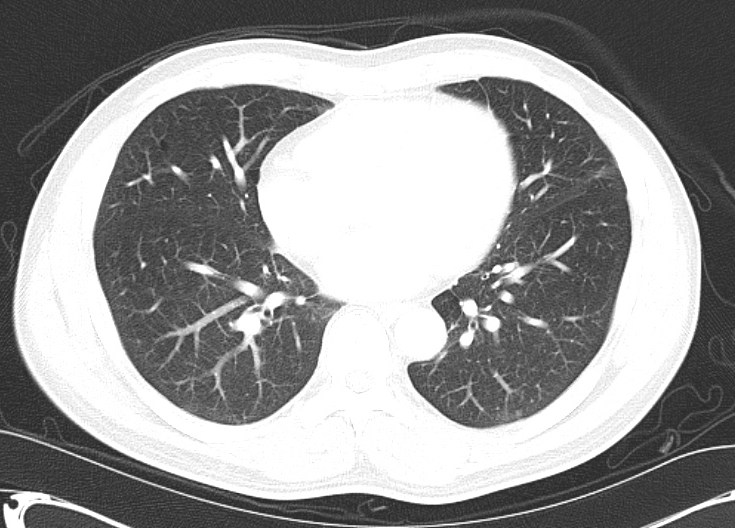
Lung Window
Switch to lung window to evaluate the lung parenchyma and continue through the abdomen to identify intraperitoneal free air
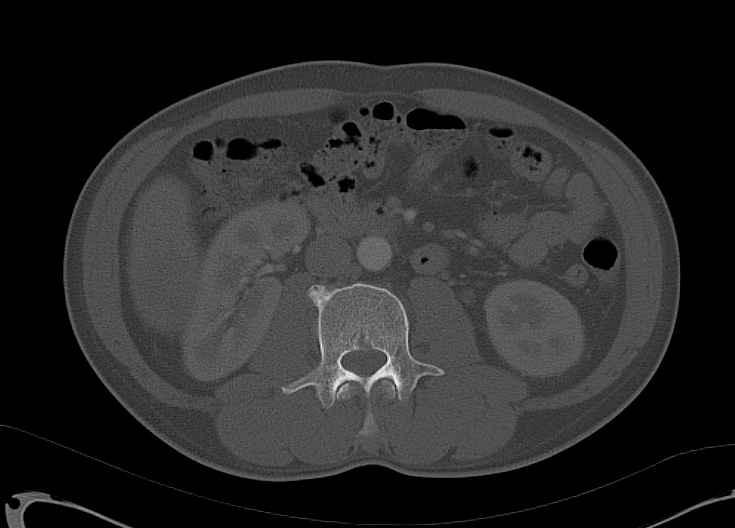
Bone Window
Use the bone window to identify fractures or lytic lesions
Try It Yourself









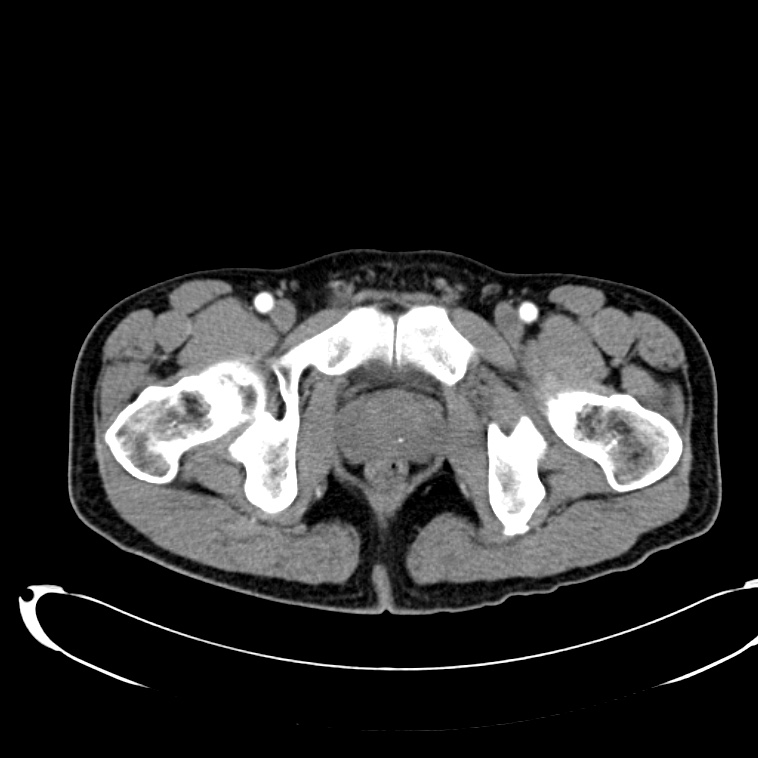
CT Abdomen/Pelvis Interpretation
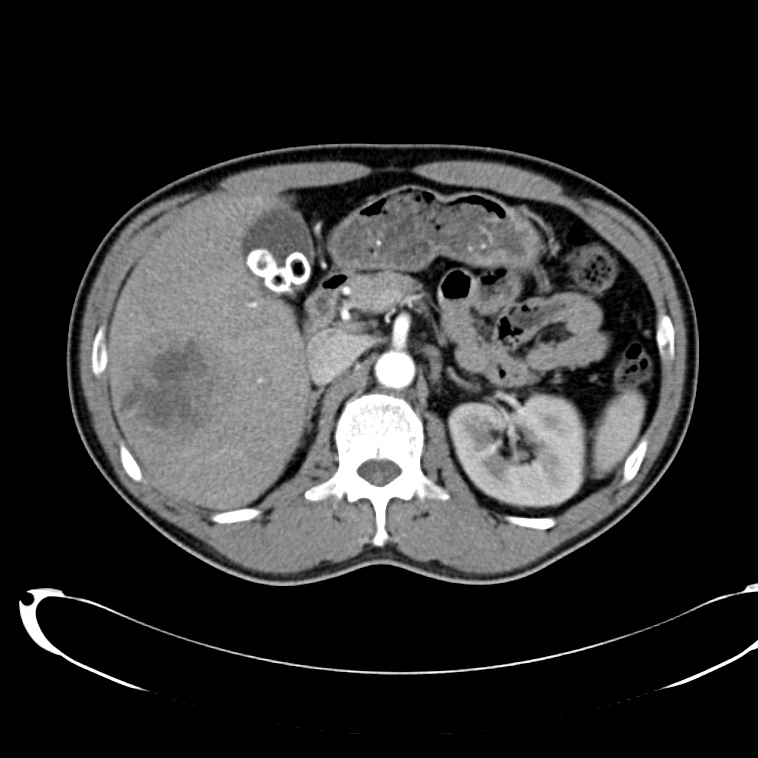
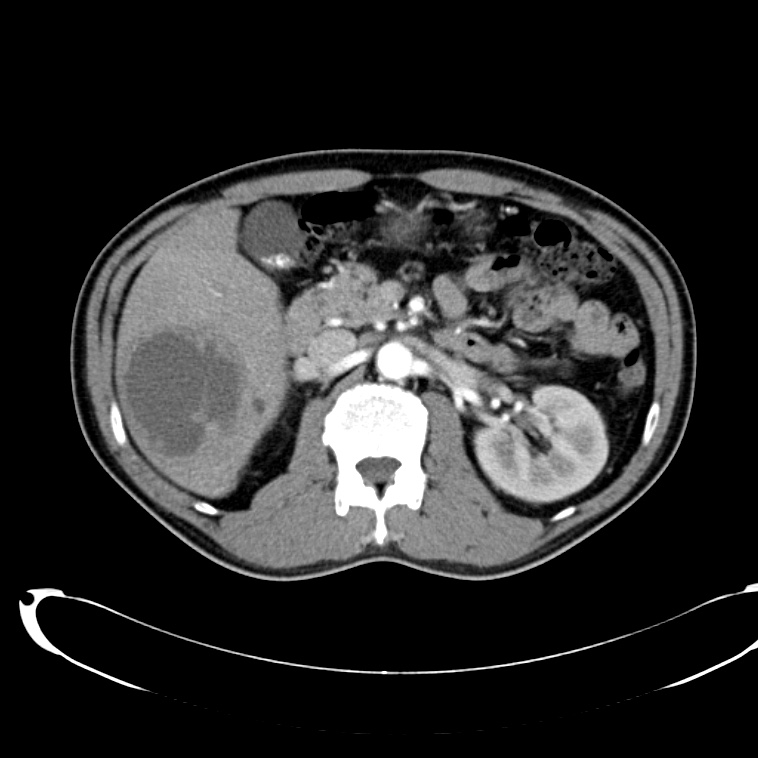
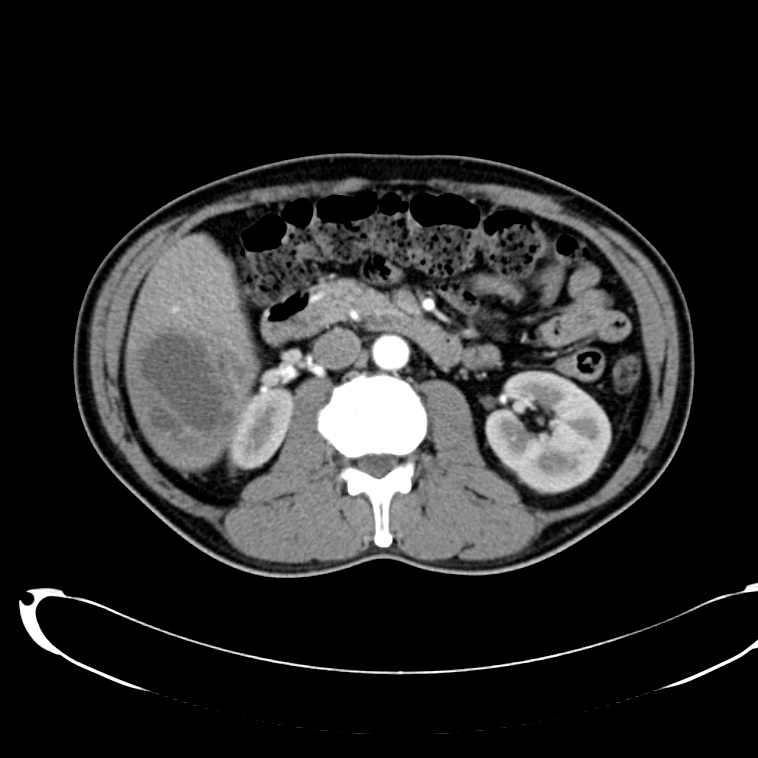
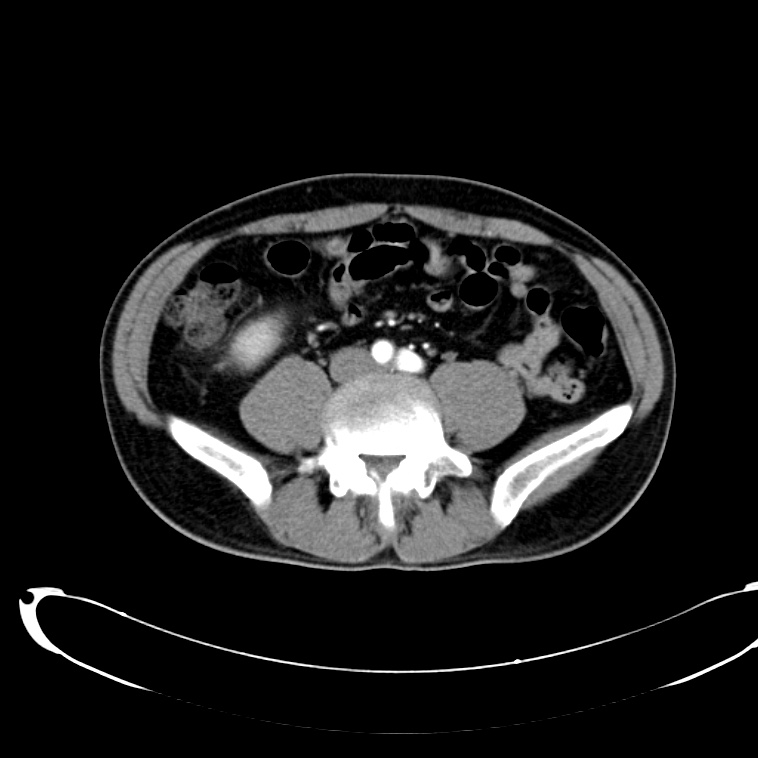
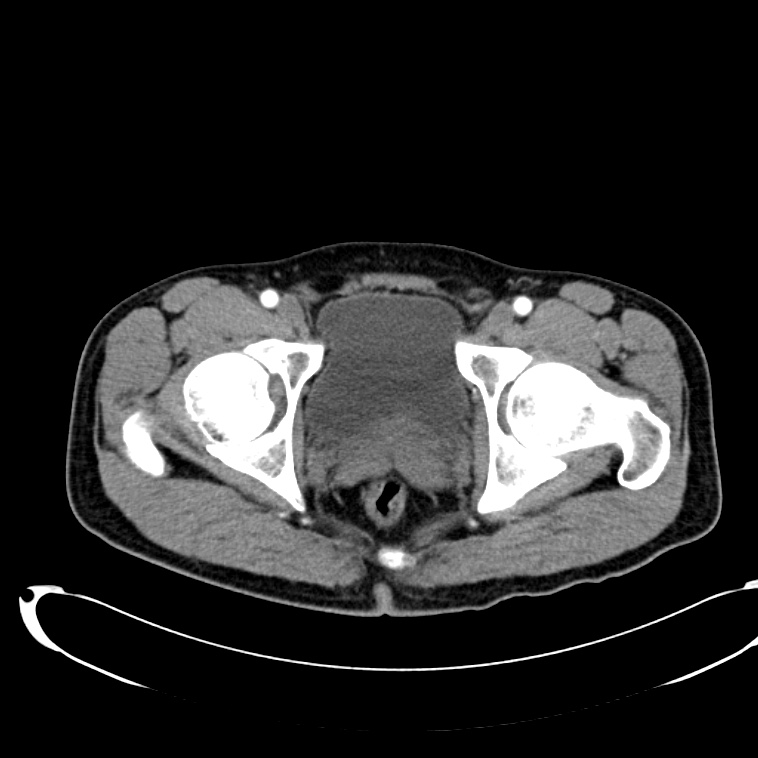
- Cystic lesion in the inferior right lobe of the liver most consistent with hepatic abscess.
- Multiple calcified gallstones in the gallbladder.