The format of this article is atypical for the structure and concept of the website – but it’s always been about learning. Here is a simplified guide to ECG interpretation with a focus on the aspects I find more challenging to understand or recall.
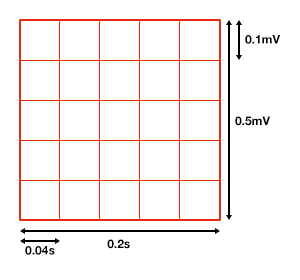
Grid and Leads
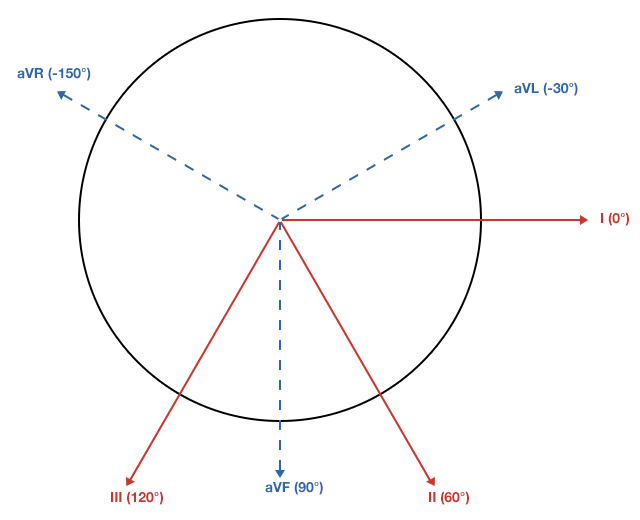
Axis

Atrial Enlargement

- Normal:
- First portion of deflection is RA, second is LA
- Right Atrial Enlargement:
- P-wave amplitude > 2.5mm in inferior leads
- Normal duration P-wave
- Left Atrial Enlargement:
- P-wave duration increased (terminal negative portion >0.04s)
- Amplitude of terminal negative component >1mm below isoelectric line in V1
Ventricular Hypertrophy
- Right Ventricular Hypertrophy:
- Right axis deviation
- Abnormal R-wave progression
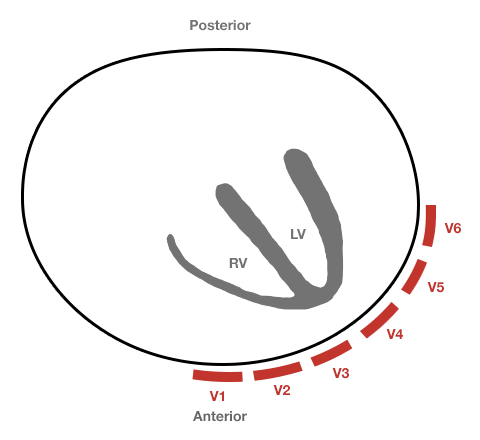
- Increased R-wave amplitude in leads overlying the right ventricle (V1)
- Increased S-wave amplitude in leads overlying the left ventricle (V6)
- Criteria
- V1: R>S
- V6: S>R
- Left Ventricular Hypertrophy:
- Left axis deviation
- Increased R-wave amplitude in leads overlying the LV (I, aVL, V5, V6)
- Increased S-wave amplitude in leads overlying the RV (V1)
- Criteria:
- Precordial Leads
- R-wave in V5/V6 + S-wave in V1/V2 > 35mm
- R-wave in V5 > 26mm
- R-wave in V6 > 20mm
- Limb Leads
- R-wave in aVL > 11mm
- R-wave in aVF > 20mm
- Combined
- R-wave in aVL + S-wave in V3 > 20mm (F), 28mm (M)
- Precordial Leads
Secondary Repolarization Abnormalities

- Downsloping ST-segment depression
- Asymmetric T-wave inversion
Bundle Branch Blocks
Left Bundle Branch Block

- QRS duration > 0.12s (3 boxes)
- Broad or notched R-wave with prolonged upstroke in I, aVL, V5, V6
- Associated ST-segment depression and T-wave inversion
- Reciprocal changes in V1, V2 (deep S-wave)
- Possible LAD
Right Bundle Branch Block

- QRS duration > 0.12s (3 boxes)
- RSR’ in V1, V2
- Reciprocal changes in I, aVL, V5, V6 (deep S-wave)
Hemiblocks

Other Blocks
- Non-specific intraventricular conduction delay: QRS >0.10s without BBB
- Incomplete BBB: LBBB/RBBB pattern with non-prolonged QRS
- Bifascicular block: RBBB + LAFB/LPFB (by axis deviation)
Ischemia and Infarction

- Hyperacute T-waves
- T-wave inversion: Symmetric, compared to TWI associated with repolarization abnormalities
- ST-elevation: Unlike J-point elevation, ST-segment merges with T-wave
- Q-waves
- Duration > 0.04s
- Amplitude > 1/3 R-wave
- Normal in aVR
Coronary Artery Territories

| Distribution | Coronary Artery | Leads | Reciprocal Changes |
|---|---|---|---|
| 1. Inferior | RCA, PDA | II, III, aVF | Anterior, Lateral |
| 2. Lateral | LCx | I, aVL, V5, V6 | Inferior |
| 3. Anterior | LAD | V1-V6 | Inferior |
| 4. Posterior | RCA | Posterior | Anterior (esp. V1) |