Brief H&P:
A 67 year-old male with a history of hypertension and diabetes presents to the emergency department after a syncopal episode. He had been completing his normal morning routine when he developed a sensation of lightheadedness and awoke on the ground of his kitchen. He denies associated chest pain, palpitations, diaphoresis, or recent illness. He has no known sick contacts nor exposures to individuals undergoing evaluation for COVID-19.
On arrival in the emergency department, the patient was noted to be hypoxic with pulse oximetry measuring 74%. He was placed on supplemental oxygen via non-rebreather with improvement of oxygen saturation to 94%. Examination demonstrated diminished alertness (requiring constant stimulation for responses) and generalized motor weakness. Cardiac and pulmonary examinations were unremarkable with the exception of tachypnea and no extremity edema was appreciated.
A chest radiograph was obtained which demonstrated platelike atelectasis. An arterial blood gas was obtained with PaO2 of 72mmHg suggesting a prominent A-a gradient. CT pulmonary angiography was obtained:




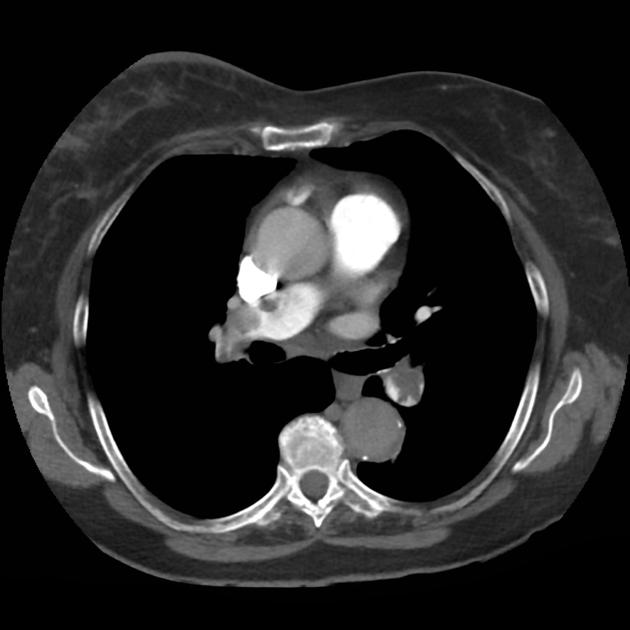


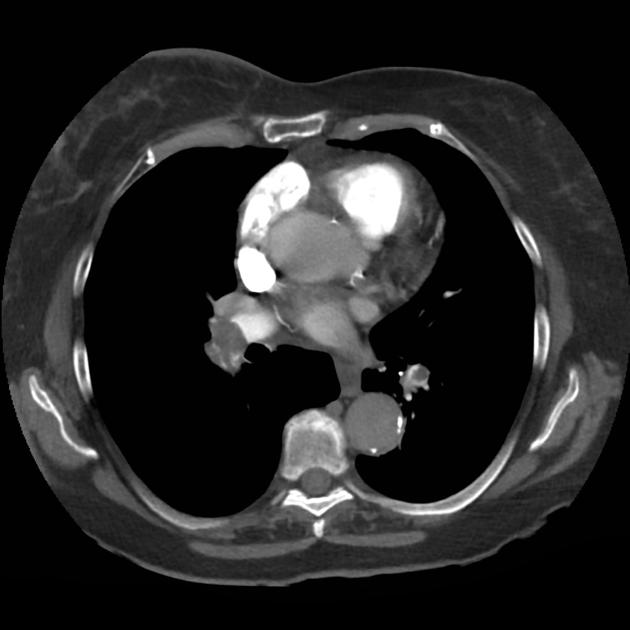


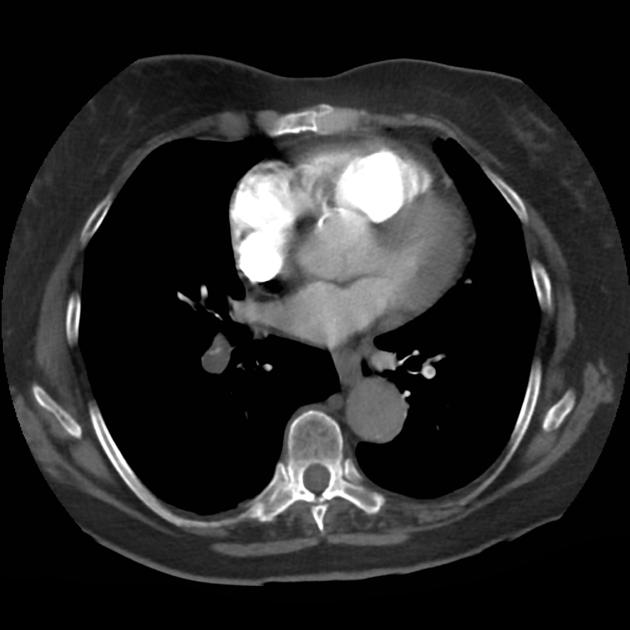
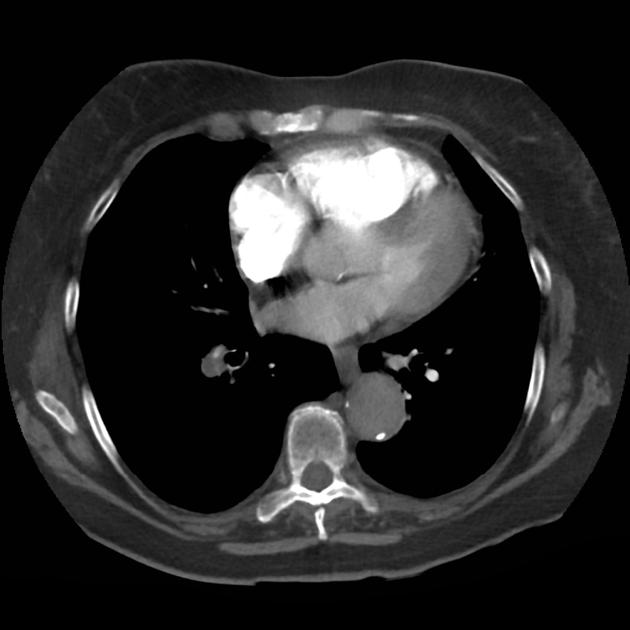
CT Pulmonary Angiography:
Bilateral pulmonary emboli. Case courtesy of Associate Prof Frank Gaillard, Radiopaedia.org, rID: 19636
Upon return, the patient’s mental status worsened associated with hypotension and he was intubated for airway protection and received systemic thrombolysis. He was subsequently taken for emergent endovascular treatment of massive pulmonary embolus.
An Algorithm for the Differential Diagnosis of Hypoxemia & Hypoxia1-7
Hypoxemia is defined as low PaO2 while hypoxia is insufficient global or local tissue oxygen content.

References
- Stapczynski J. Respiratory Distress. In: Tintinalli JE, Ma O, Yealy DM, Meckler GD, Stapczynski J, Cline DM, Thomas SH. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com/content.aspx?bookid=2353§ionid=219642010. Accessed April 12, 2020.
- Gas Transport & pH. In: Barrett KE, Barman SM, Brooks HL, Yuan JJ. eds. Ganong’s Review of Medical Physiology, 26e New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com/content.aspx?bookid=2525§ionid=204297654. Accessed April 12, 2020.
- Loscalzo J. Hypoxia and Cyanosis. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 20e New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com/content.aspx?bookid=2129§ionid=192012521. Accessed April 12, 2020.
- West NE, Lechtzin N. Chapter 93. Hypoxia. In: McKean SC, Ross JJ, Dressler DD, Brotman DJ, Ginsberg JS. eds. Principles and Practice of Hospital Medicine New York, NY: McGraw-Hill; 2012. http://accessmedicine.mhmedical.com/content.aspx?bookid=496§ionid=41304065. Accessed April 12, 2020.
- Pulmonary Physiology. In: Kibble JD, Halsey CR. eds. Medical Physiology: The Big Picture New York, NY: McGraw-Hill; 2014. http://accessmedicine.mhmedical.com/content.aspx?bookid=1291§ionid=75576764. Accessed April 12, 2020.
- Petersson, J., Glenny, R. (2014). Gas exchange and ventilation–perfusion relationships in the lung European Respiratory Journal 44(4), 1023-1041. https://dx.doi.org/10.1183/09031936.00037014
- Morchi, R. (2011). Diagnosis Deconstructed: The Case of the Patient with No Chief Complaint Emergency Medicine News XXXIII(3)
Rodríguez-Roisin, R., Roca, J. (2005). Mechanisms of hypoxemia Intensive Care Medicine 31(8), 1017-1019. https://dx.doi.org/10.1007/s00134-005-2678-1