HPI:
34 year-old male brought in by ambulance s/p assault. Field GCS reportedly 7, in trauma bay assessed as E2-V4-M6. Witnessed seizure in CT scanner, resolved with lorazepam. Intubated for airway protection, underwent external ventricular drain placement and transferred to surgical ICU.
Initial imaging revealed bifrontal subdural hematomas and right temporal hemorrhagic contusion with generalized edema. Repeat imaging one hour later showed interval development of large extra-axial hemorrhage overlying the right occipital and parietal lobes (2.2cm), representing subdural or epidural hematoma.
The patient’s ICU course was complicated by continued seizures and refractory elevation in intracranial pressure. A pentobarbital infusion was started and titrated to adequate burst suppression and hyperosmolar therapy with both mannitol and hypertonic saline continued. Additional imaging revealed stable hemorrhage but continued diffuse cerebral edema evidenced by sulcal effacement.
On hospital day 5, examination revealed bilateral fixed and dilated pupils. Imaging revealed effacement of basilar cisterns, pre-pontine cistern, and cisterna magna suggestive of impending/ongoing transtentorial and tonsillar herniation. Pentobarbital was weaned and conventional cerebral angiography as well as cerebral perfusion studies were consistent with brain death.
Images



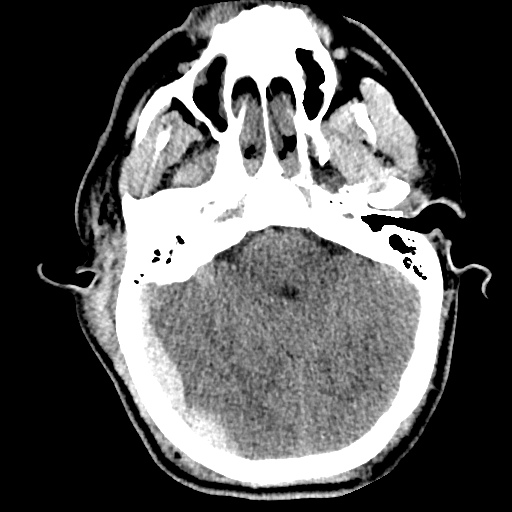





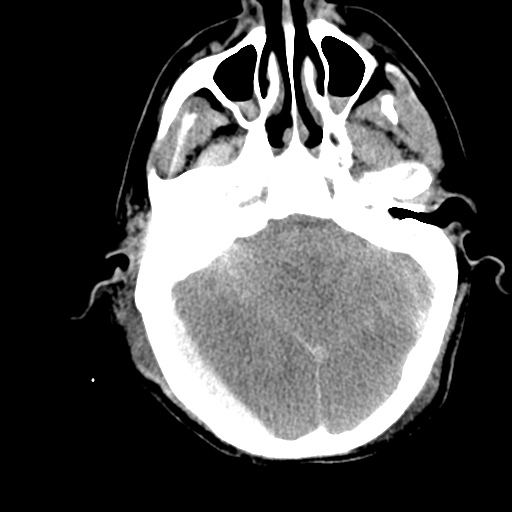
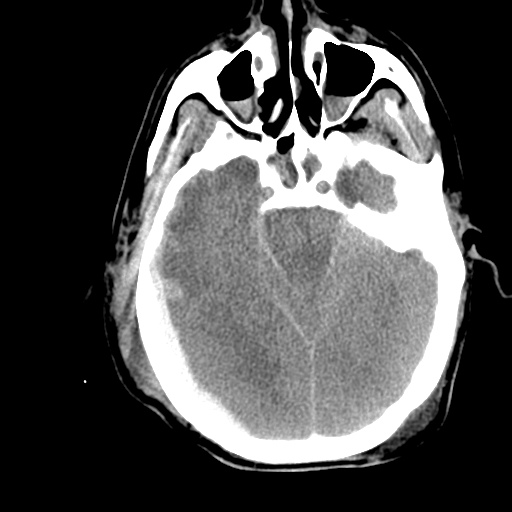
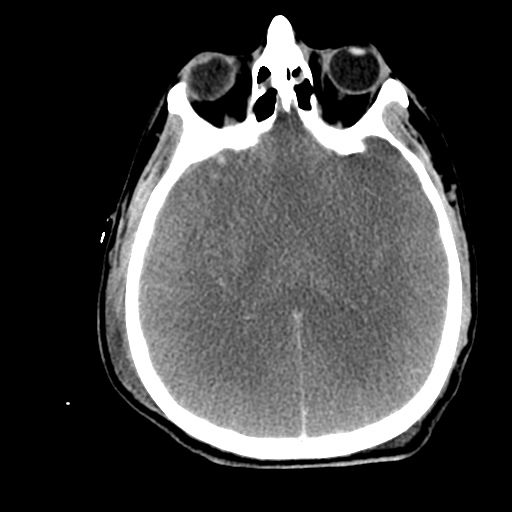
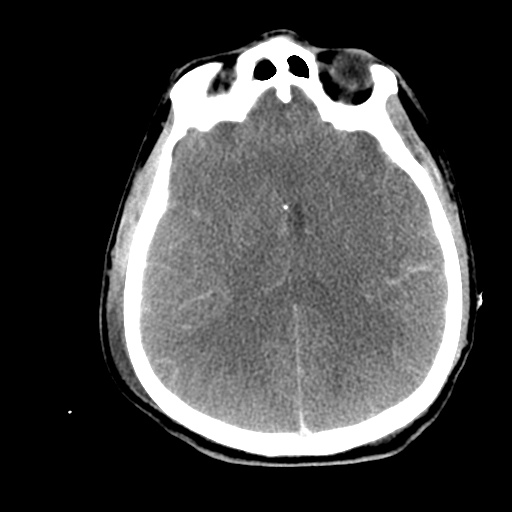
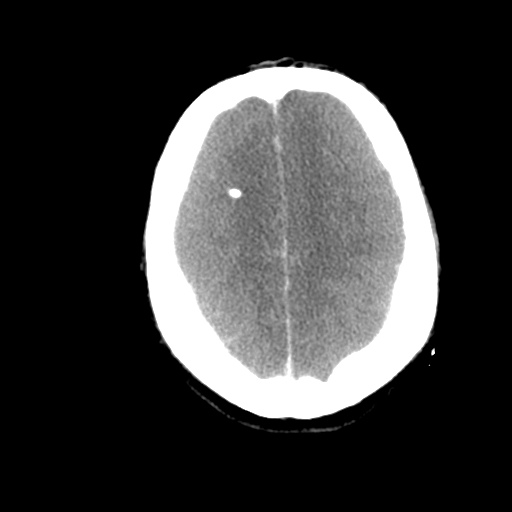
CT head without contrast one hour after presentation
- Large extra-axial posterior hemorrhages. Hemorrhagic contusions in the right frontal and temporal lobes.
- The cerebral sulci appear effaced – findings suggest diffuse cerebral edema.
- S/p EVD using a right frontal approach.


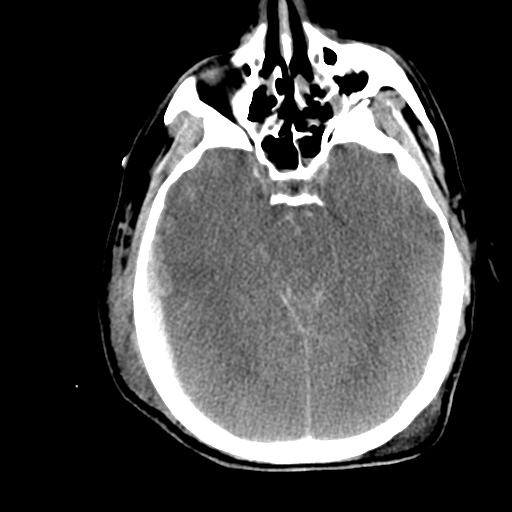
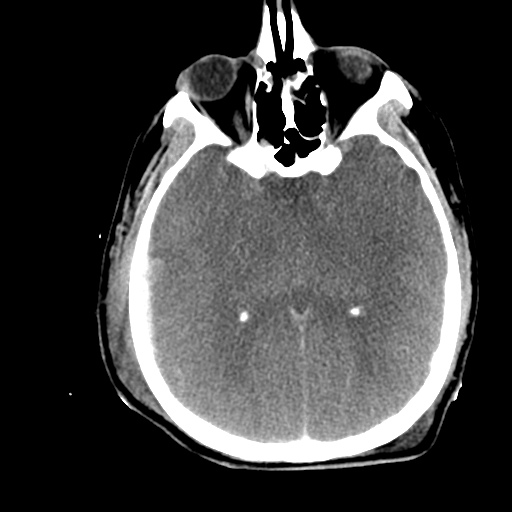
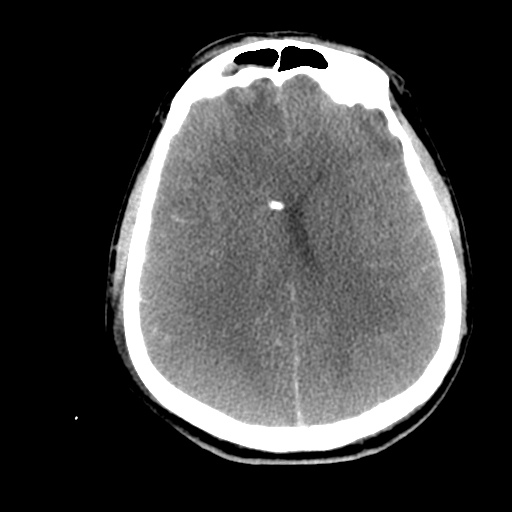
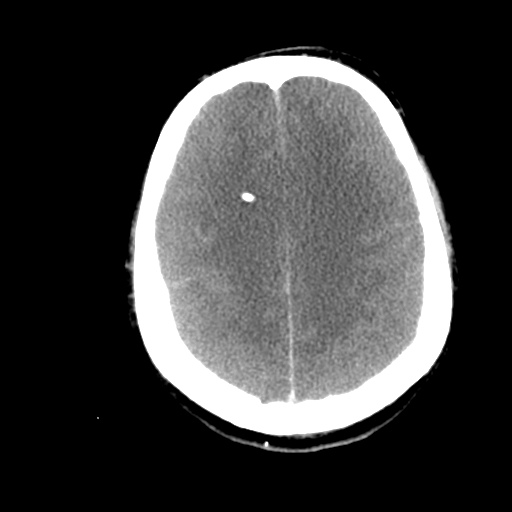
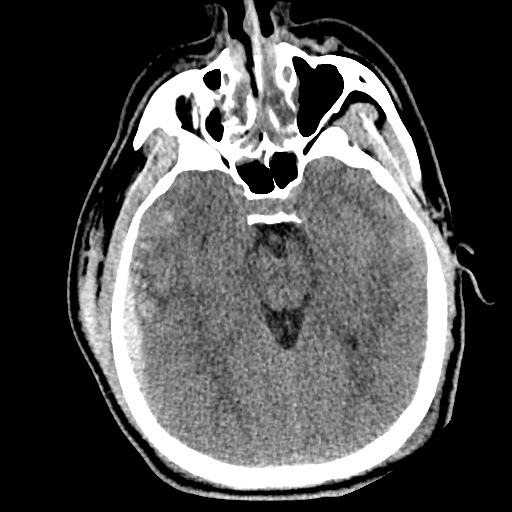
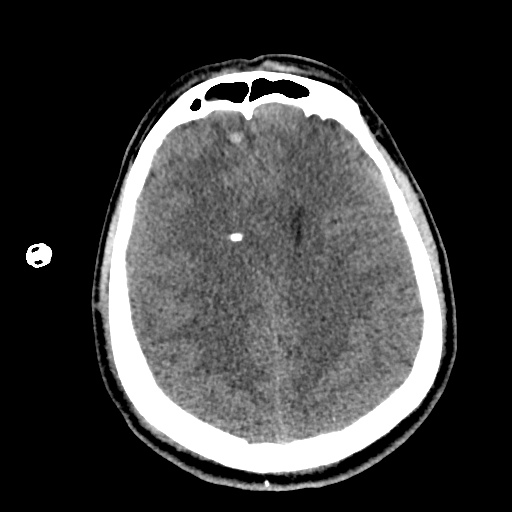
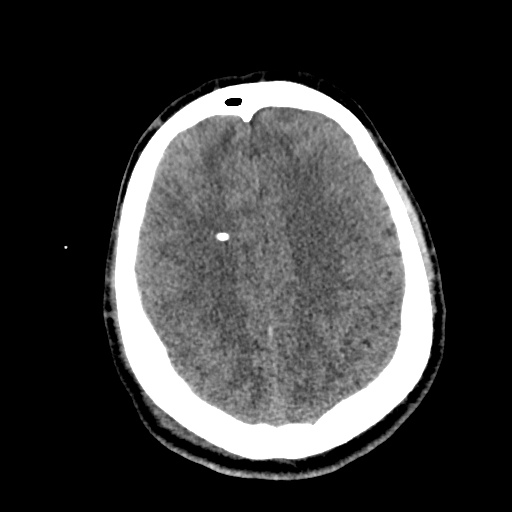
CT head without contrast on hospital day 5
- Interval evidence of global hypoxic/ischemic injury to the brain.
- Interval apparent effacement of the basilar cisterns, pre-pontine cistern, and cisterna magna suggesting impending/ongoing downward transtentorial herniation and tonsillar herniation.
- Stable supra/infratentorial subdural/epidural hematoma.
Algorithm for the Management of Severe Traumatic Brain Injury1,2

References
- Brain Trauma Foundation, American Association of Neurological Surgeons, Congress of Neurological Surgeons, Joint Section on Neurotrauma and Critical Care, AANS/CNS, Carney, N. A., & Ghajar, J. (2007). Guidelines for the management of severe traumatic brain injury. Introduction. Journal of neurotrauma, 24 Suppl 1, S1–2. doi:10.1089/neu.2007.9997
- Stocchetti, N., & Maas, A. I. R. (2014). Traumatic intracranial hypertension. The New England journal of medicine, 370(22), 2121–2130. doi:10.1056/NEJMra1208708
- WikEM: Severe traumatic brain injury