Brief HPI:
An approximately 70 year-old male with unknown medical history is brought to the emergency department with altered mental status. A community member contacted police after not seeing the patient for the past three days which was unusual. Upon entering the patient’s home, EMS found the patient on the ground, unresponsive. Capillary glucose was normal and naloxone was administered without appreciable effect.
On arrival in the emergency department, the patient remained unresponsive to verbal and noxious stimulation and was intubated for airway protection. Vital signs were notable for hypotension (BP 88/45mmHg) and a core temperature of 96.5°F. Physical examination demonstrated cool extremities and ecchymosis and edema involving the right upper and lower extremities. The patient’s blood pressure improved with fluid resuscitation and empiric broad-spectrum antibiotics were administered due to concern for infection in the setting of hypothermia.
Laboratory/Imaging Results
Laboratory tests were notable for leukocytosis and creatine kinase above the threshold for detection. Radiology preliminary interpretation of non-contrast head imaging was normal. A lumbar puncture was performed with grossly purulent cerebrospinal fluid.
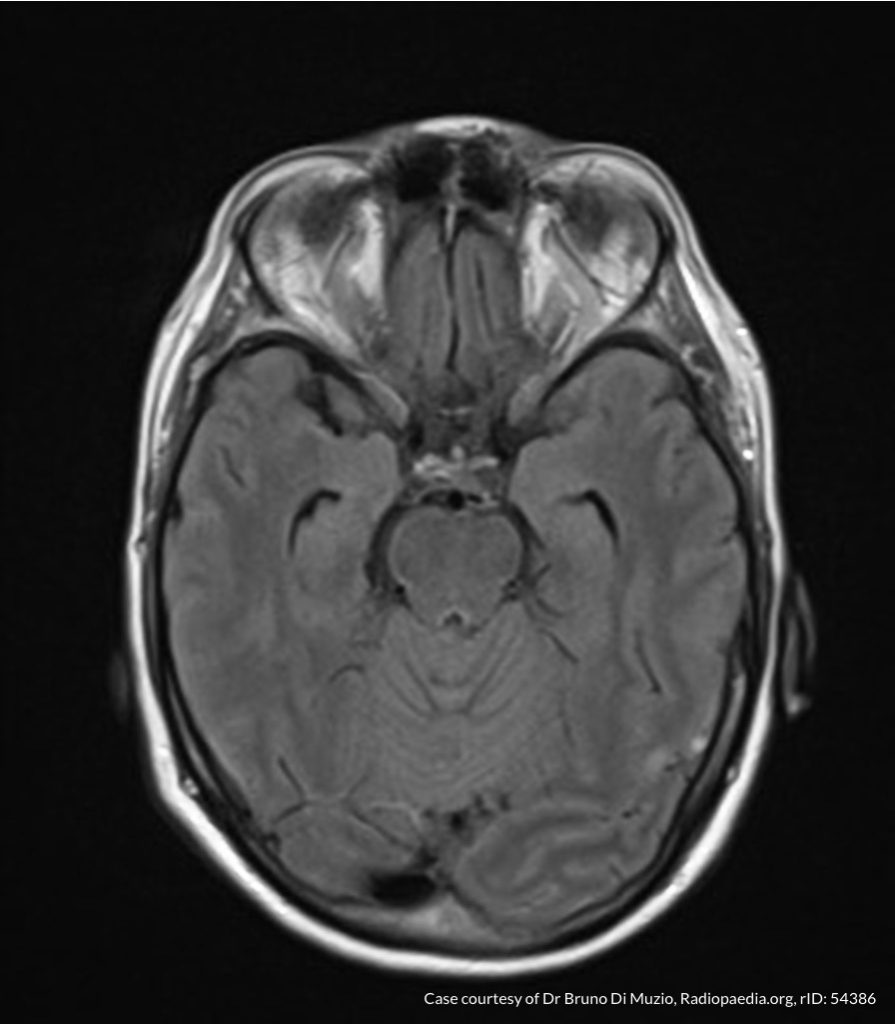
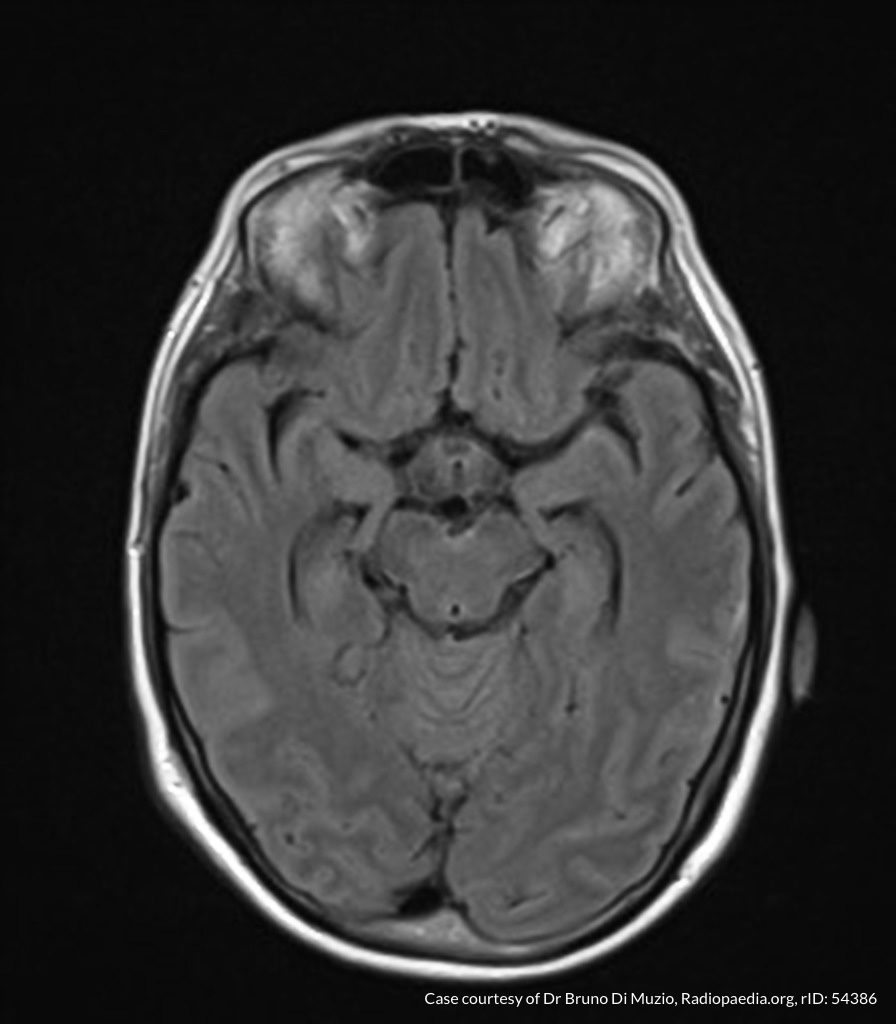
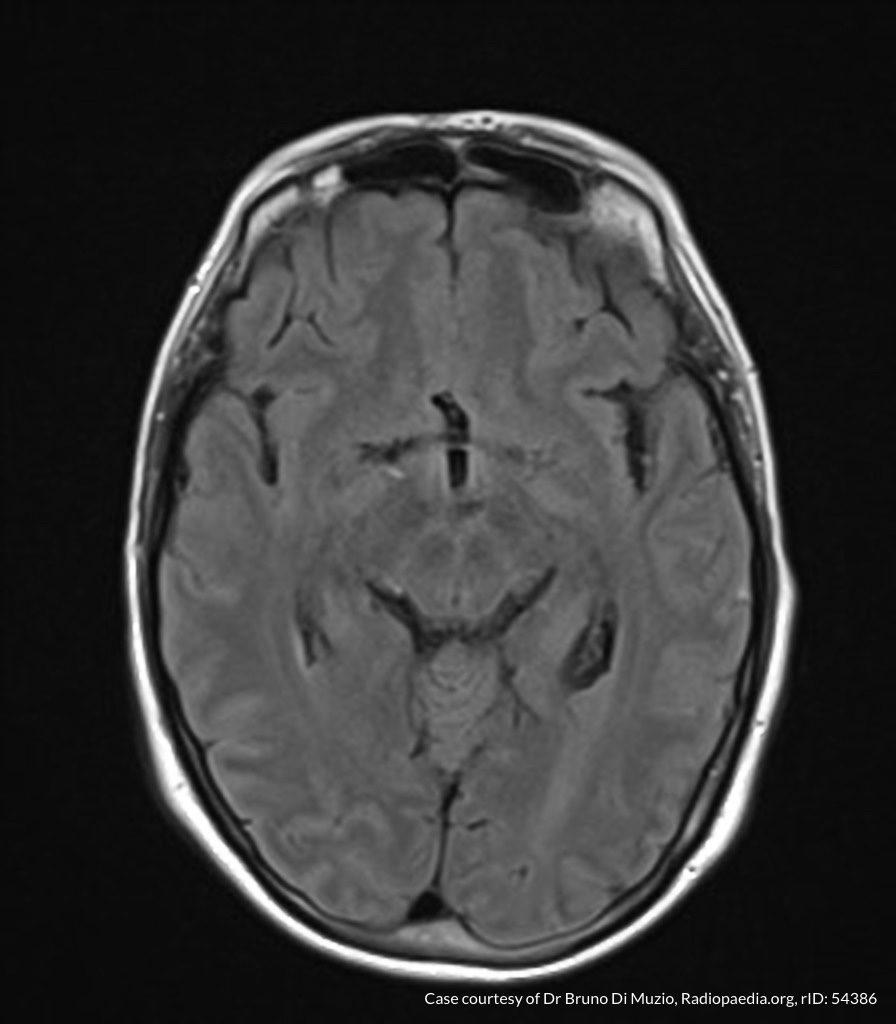
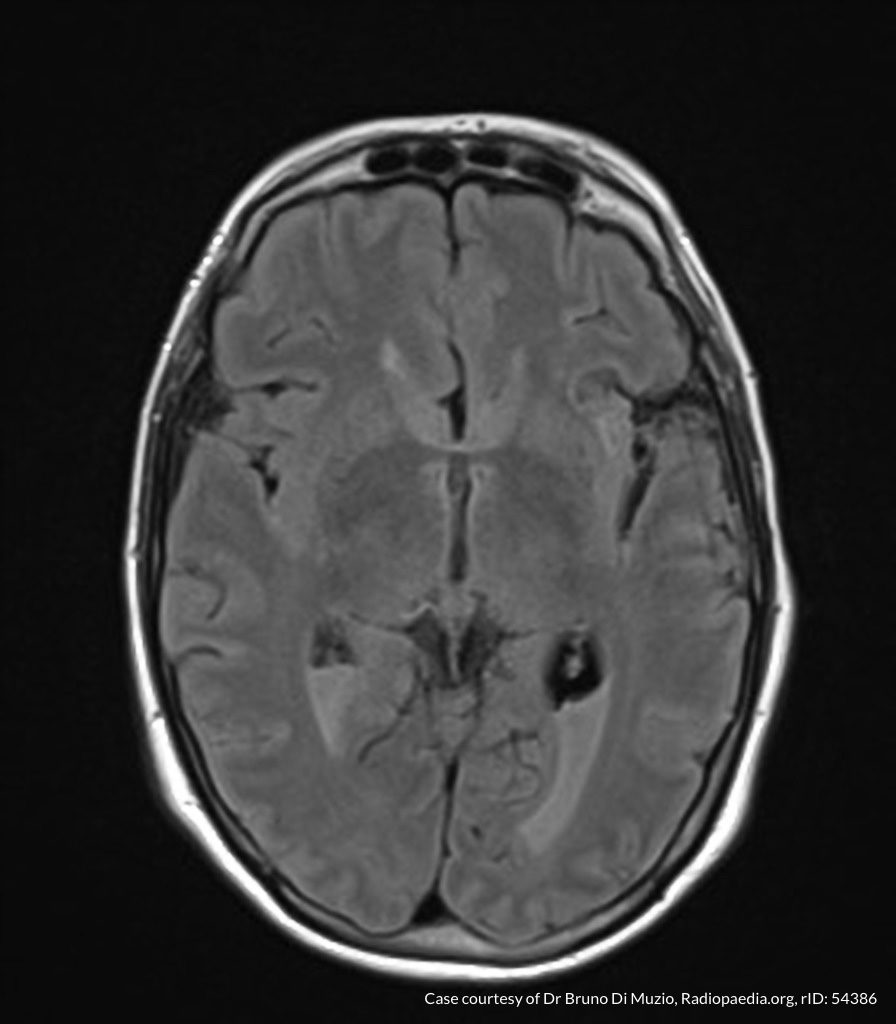
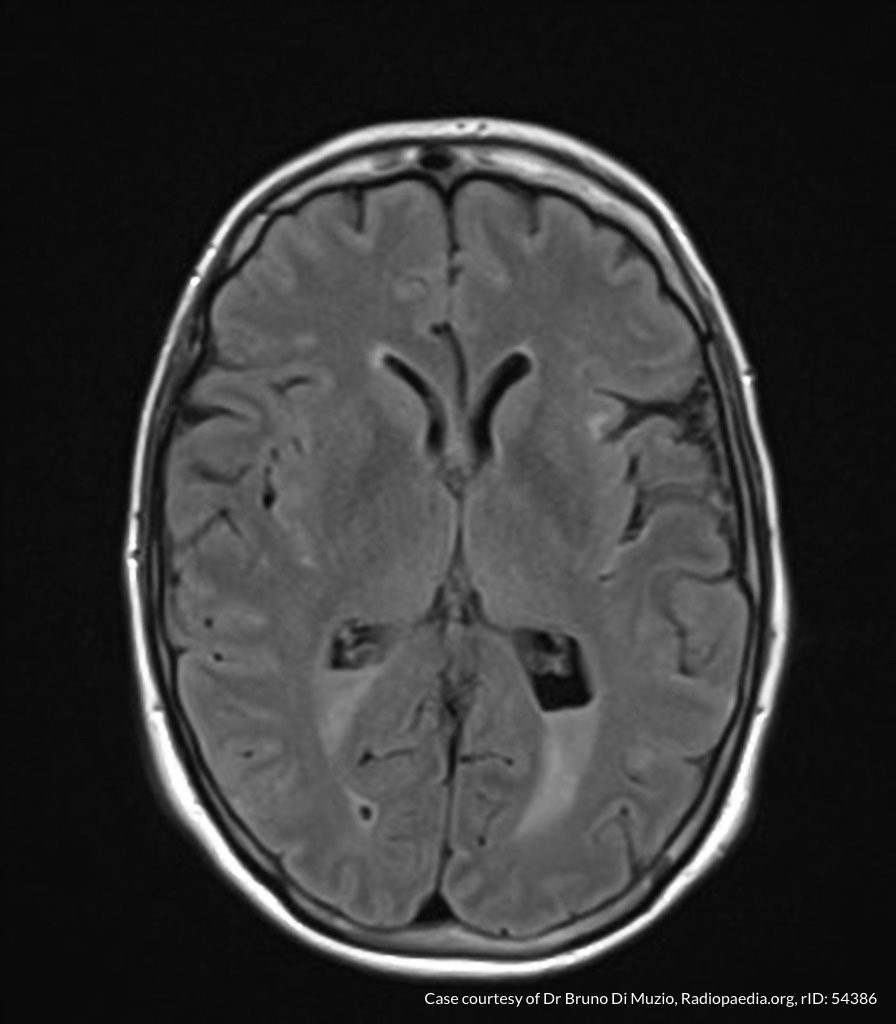
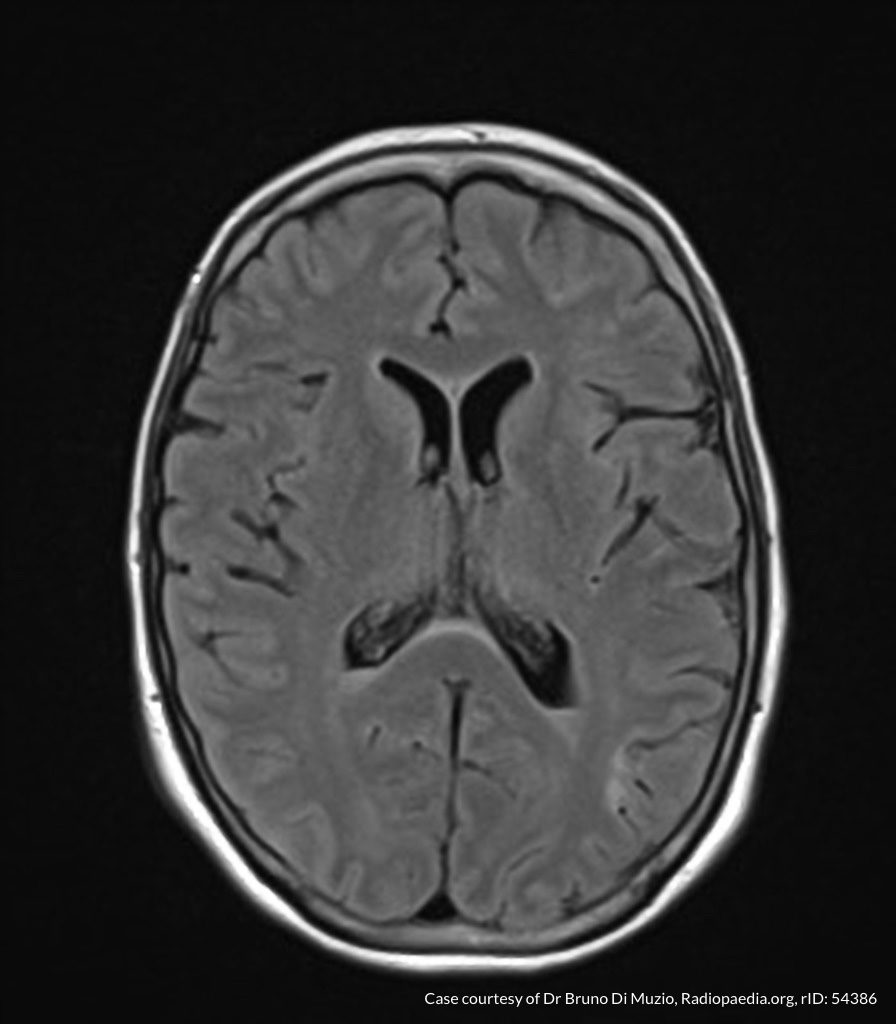
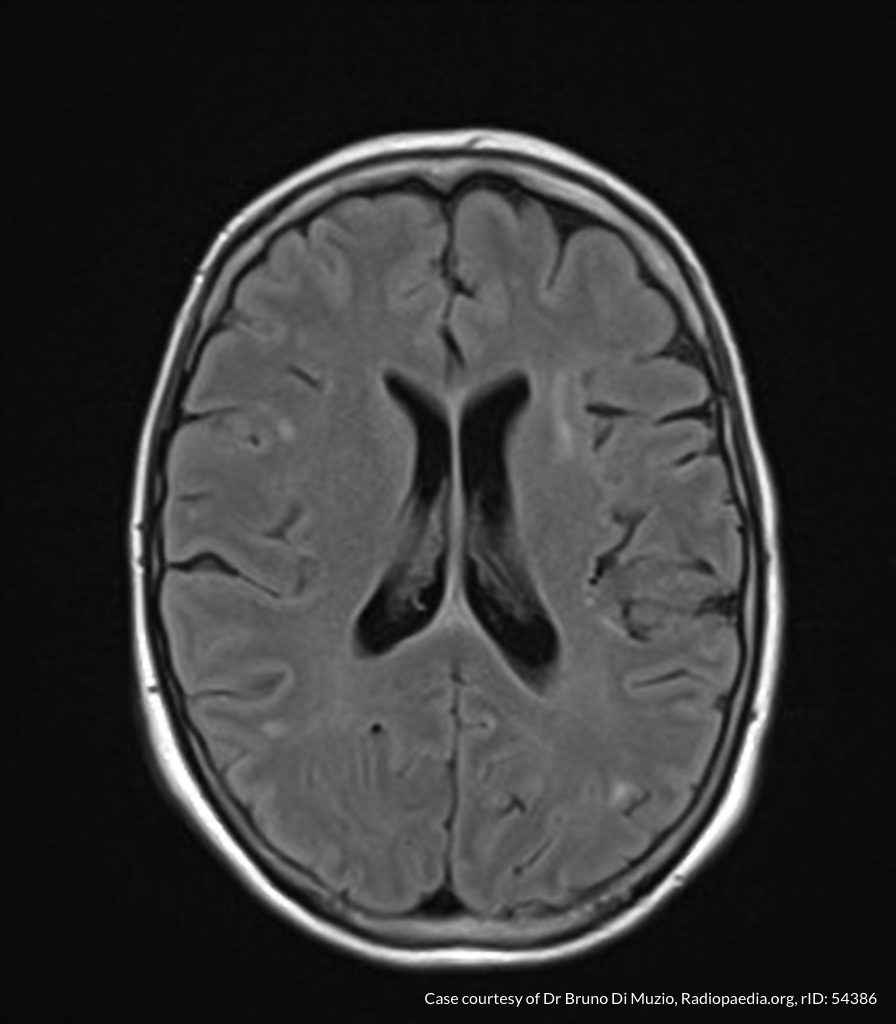
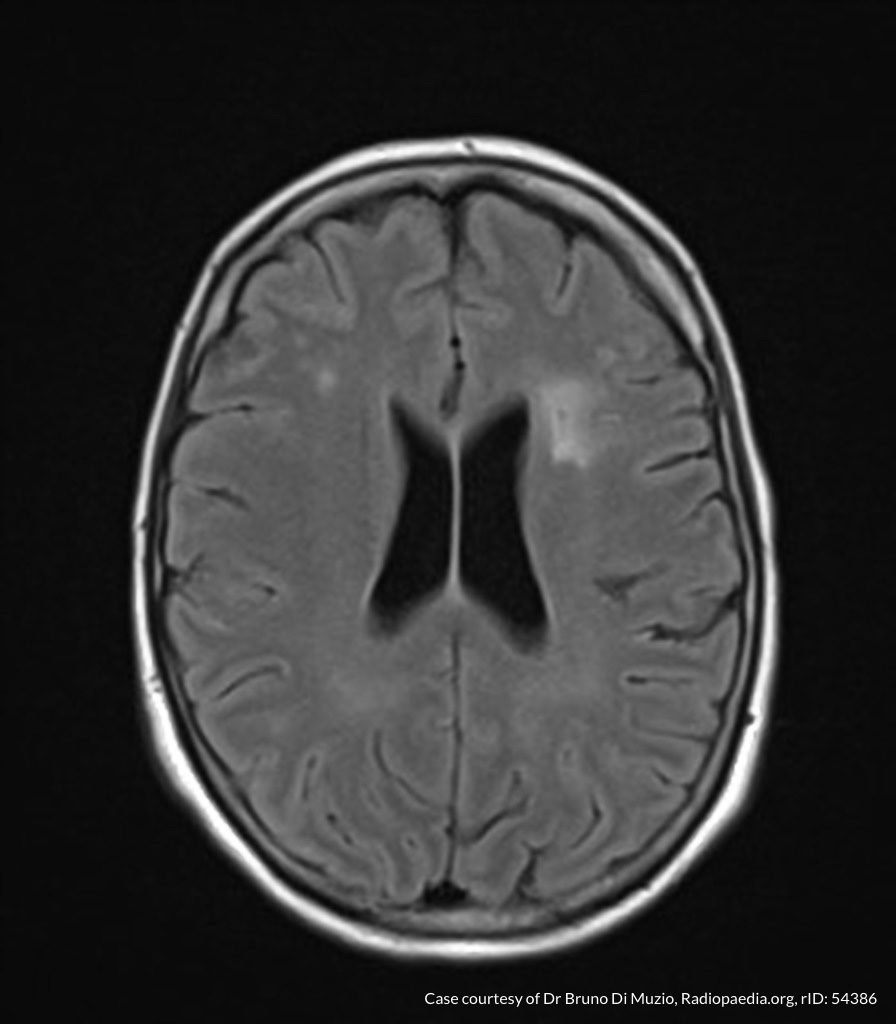
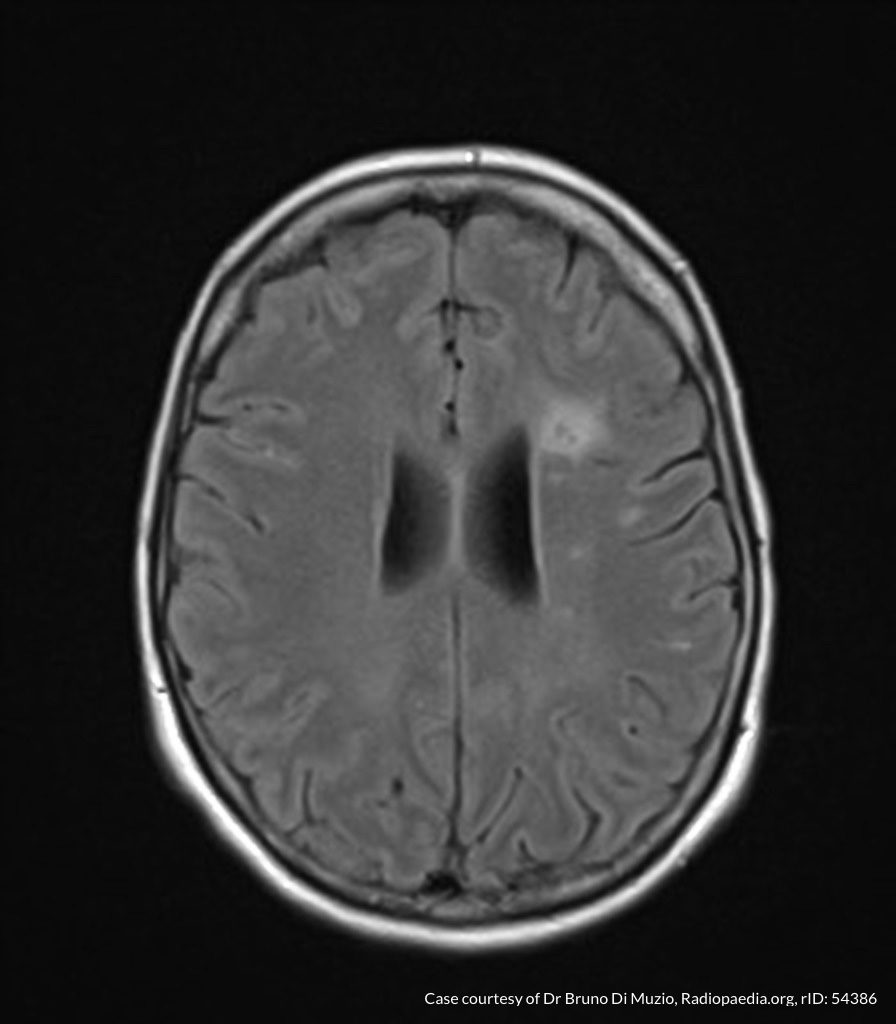
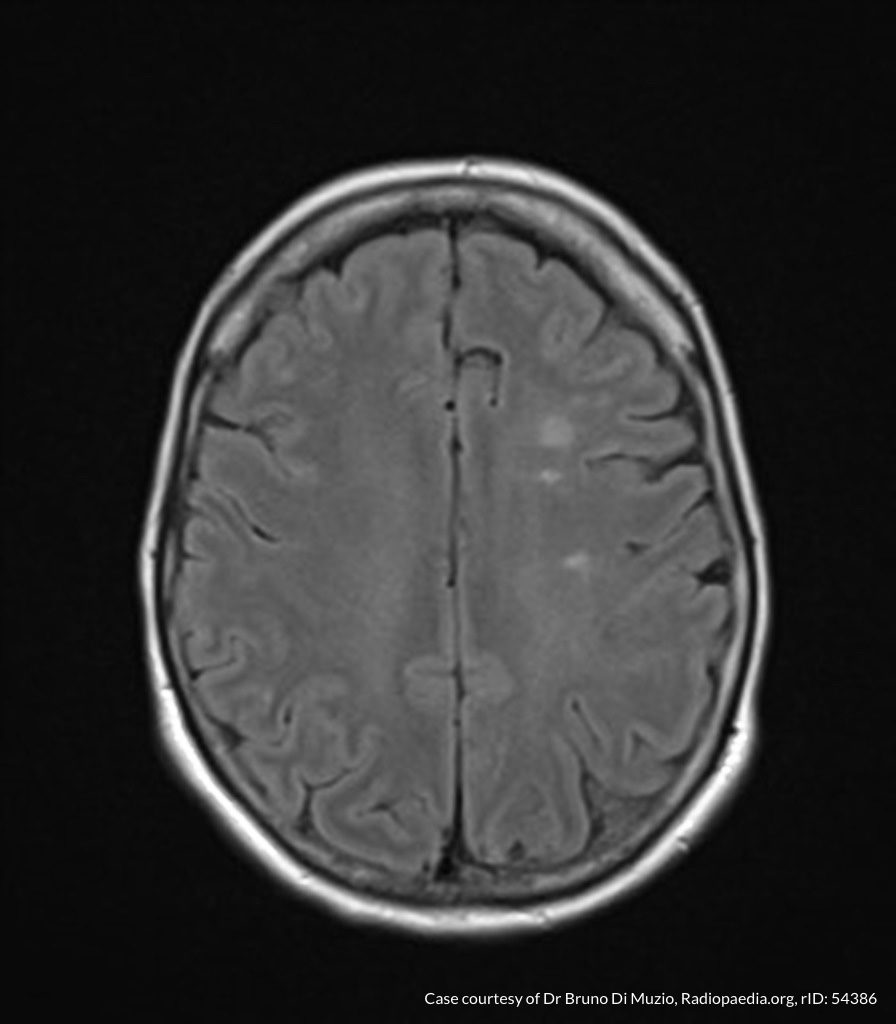
MRI Brain
Dependent material within the occipital horns of the lateral ventricles consistent with ventriculitis.
Hospital Course
The patient was admitted for the treatment of presumed meningitis. Radiology final interpretation of non-contrast head computed tomography commented on ventricular debris suggestive of ventriculitis which was later confirmed on magnetic resonance imaging1,2. Due to poor response to systemic antibiotics, neurosurgery was consulted, a ventricular drain was placed with administration of intrathecal antibiotics. The patient’s condition continued to deteriorate and family members elected to allow his natural death.
An Algorithm for the Analysis of Cerebrospinal Fluid (CSF)3-14

References
- Lesourd A, Magne N, Soares A, et al. Primary bacterial ventriculitis in adults, an emergent diagnosis challenge: report of a meningoccal case and review of the literature. BMC Infect Dis. 2018;18(1):226. doi:10.1186/s12879-018-3119-4.
- Gofman N, To K, Whitman M, Garcia-Morales E. Successful treatment of ventriculitis caused by Pseudomonas aeruginosa and carbapenem-resistant Klebsiella pneumoniae with i.v. ceftazidime-avibactam and intrathecal amikacin. Am J Health Syst Pharm. 2018;75(13):953-957. doi:10.2146/ajhp170632.
- Dorsett M, Liang SY. Diagnosis and Treatment of Central Nervous System Infections in the Emergency Department. Emerg Med Clin North Am. 2016;34(4):917-942. doi:10.1016/j.emc.2016.06.013.
- Perry JJ, Alyahya B, Sivilotti MLA, et al. Differentiation between traumatic tap and aneurysmal subarachnoid hemorrhage: prospective cohort study. BMJ. 2015;350:h568. doi:10.1136/bmj.h568.
- Lee SCM, Lueck CJ. Cerebrospinal fluid pressure in adults. J Neuroophthalmol. 2014;34(3):278-283. doi:10.1097/WNO.0000000000000155.
- Brouwer MC, Thwaites GE, Tunkel AR, van de Beek D. Dilemmas in the diagnosis of acute community-acquired bacterial meningitis. Lancet. 2012;380(9854):1684-1692. doi:10.1016/S0140-6736(12)61185-4.
- Wright BLC, Lai JTF, Sinclair AJ. Cerebrospinal fluid and lumbar puncture: a practical review. J Neurol. 2012;259(8):1530-1545. doi:10.1007/s00415-012-6413-x.
- Gorchynski J, Oman J, Newton T. Interpretation of traumatic lumbar punctures in the setting of possible subarachnoid hemorrhage: who can be safely discharged? Cal J Emerg Med. 2007;8(1):3-7.
- Deisenhammer F, Bartos A, Egg R, et al. Guidelines on routine cerebrospinal fluid analysis. Report from an EFNS task force. Eur J Neurol. 2006;13(9):913-922. doi:10.1111/j.1468-1331.2006.01493.x.
- Seehusen DA, Reeves MM, Fomin DA. Cerebrospinal fluid analysis. Am Fam Physician. 2003;68(6):1103-1108.
- Shah KH, Edlow JA. Distinguishing traumatic lumbar puncture from true subarachnoid hemorrhage. J Emerg Med. 2002;23(1):67-74.
- Walker HK, Hall WD, Hurst JW. Clinical Methods: The History, Physical, and Laboratory Examinations. 1990.
- Mayefsky JH, Roghmann KJ. Determination of leukocytosis in traumatic spinal tap specimens. Am J Med. 1987;82(6):1175-1181.
- Geiseler PJ, Nelson KE, Levin S, Reddi KT, Moses VK. Community-acquired purulent meningitis: a review of 1,316 cases during the antibiotic era, 1954-1976. Rev Infect Dis. 1980;2(5):725-745.
Pingback: Differential Diagnosis of Headache