HPI:
32F G8P7A2 at 5 weeks by LMP presenting with abdominal pain. The patient reports acute onset of sharp left lower abdominal pain 1.5 hours prior to presentation. The pain has been constant since onset, 10/10 in severity, radiating to lower back and exacerbated with movement. She denies vaginal bleeding or discharge, passage of clots or other products. She also denies trauma, lightheadedness/dizziness/syncope, shortness of breath, nausea/vomiting or changes in bowel or urinary habits.
Her pregnancy was detected 3 weeks ago with a home pregnancy test and was confirmed at her PCP one week later. She has not had an ultrasound during this pregnancy but has a history of uterine fibroids. She has no history of sexually transmitted infections, prior ectopic pregnancy, or use of assisted fertilization.
PMH:
- HTN
- Uterine fibroids
PSH:
None
FH:
Non-contributory
SHx:
- Denies tobacco, alcohol or drug use.
- Sexually active with husband only, no history of STI.
Meds:
None
Allergies:
NKDA
Physical Exam:
| VS: | T | 37.4 | HR | 108 | RR | 36 | BP | 148/104 | O2 | 99% RA |
| Gen: | Alert and oriented female, appears uncomfortable due to pain. | |||||||||
| HEENT: | PERRL, EOMI, MMM. | |||||||||
| CV: | Tachycardia, regular rhythm, no murmurs. | |||||||||
| Lungs: | CTAB, no crackles. | |||||||||
| Abd: | Normoactive bowel sounds, tenderness to palpation in LLQ and suprapubic area, with guarding but no rebound tenderness. No CVAT. | |||||||||
| GU: | No external lesions. Closed cervical os, no blood or discharge, +CMT. | |||||||||
| Ext: | Warm, well-perfused with strong peripheral pulses. | |||||||||
Labs/Studies:
- POC Hemoglobin: 11.8
- POC ICON: positive
Imaging:
Bedside Ultrasound
- Transabdominal: Free fluid in hepatorenal and splenorenal recesses
- Transvaginal: Free fluid and debris in posterior cul-de-sac, likely pseudogestational sac in endometrial cavity, no IUP identified. Formal ultrasound revealed fetus with cardiac activity in left adnexa.

Hepatorenal free fluid
Free fluid in the hepatorenal recess (Morison's Pouch)
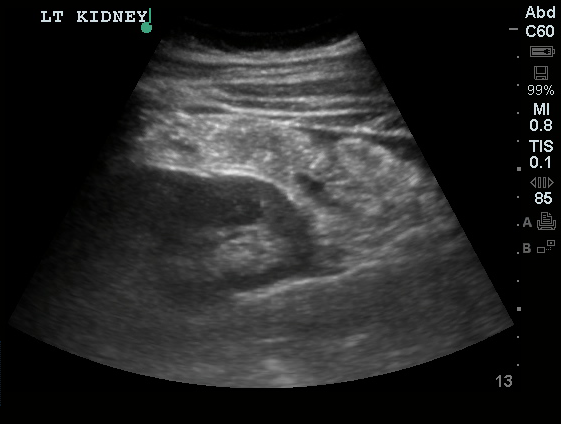
Splenorenal Free Fluid
Free fluid in the splenorenal recess.
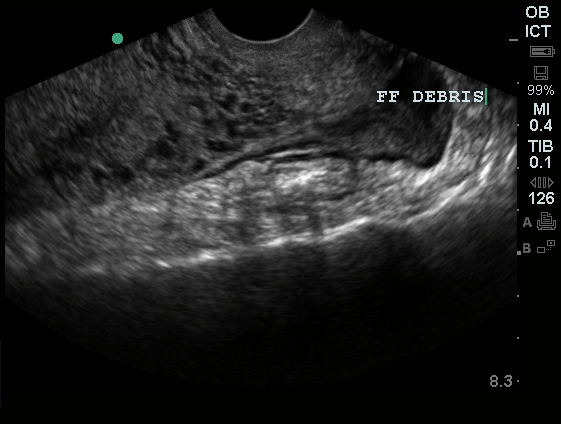
Pelvic Free Fluid
Free fluid and debris in the posterior cul-de-sac.
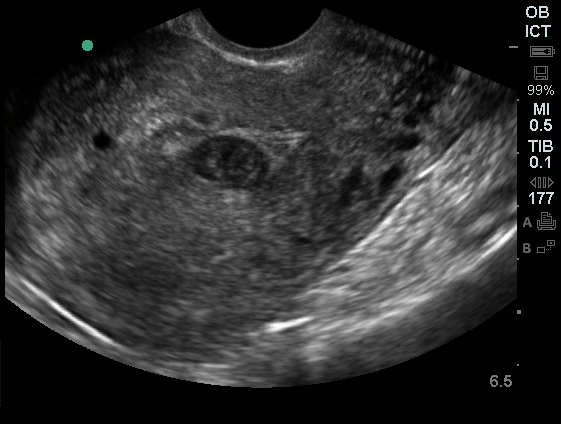
Pseudogestational Sac
No obvious yolk sac or fetal pole.
Assessment/Plan:
32 year-old ICON positive female with acute-onset pelvic pain. The patient remained hemodynamically stable and absence of definitive IUP on bedside ultrasound was confirmed with presence of fetal cardiac activity in left adnexa indicative of ectopic pregnancy. OB-Gyn was consulted and the patient was taken emergently to the OR.
Differential Diagnosis of First Trimester Abdominal Pain: 1

Initial Evaluation of First Trimester Abdominal Pain: 1
- 2 large-bore IV’s, begin fluid resuscitation
- POC testing: hemoglobin, urine pregnancy
- CBC, type and cross (Rh), serum B-hCG
- Emergent bedside ultrasound
Features Associated with Ectopic Pregnancy: 1
- PID
- Tubal ligation
- Prior ectopic
- IUD
- Assisted fertilization
- CMT
- Peritoneal irritation
- Empty uterus
- Adnexal mass
- Free fluid
Ultrasonographic Findings in the Evaluation of Ectopic Pregnancy: 2
- Discriminatory hCG (1500-3000 mIU/mL): absence of IUP suggests ectopic or abnormal gestation
- Normal IUP
- 4-5wks: gestational sac (0.2-0.5cm)
- 5wks: two echogenic rings
- 5.5wks: yolk sac
- 6wk: embryonic pole
- 6.5wk: fetal cardiac activity
- Abnormal IUP
- >2cm gestational sac without fetal pole
- CRL >0.5cm without cardiac activity
- Ectopic
- Extrauterine gestational sac with or without cardiac activity
- Extrauterine ring sign
- Non-homogenous adnexal mass
Contraindications to Medical Management: 2,3
- Absolute
- Breast-feeding
- Immunodeficiency
- PUD
- Pulmonary, hepatic or renal dysfunction
- Relative
- Ectopic mass > 3.5cm
- Fetal cardiac activity
References:
- Dart, R. (2003). First Trimester Emergencies A Practical Approach To Abdominal Pain And Vaginal Bleeding In Early Pregnancy. EB Medicine, 5(11), 1–20.
- Barnhart, K. T. (2009). Clinical practice. Ectopic pregnancy. The New England journal of medicine, 361(4), 379–387. doi:10.1056/NEJMcp0810384
- Jurkovic, D., & Wilkinson, H. (2011). Diagnosis and management of ectopic pregnancy. BMJ (Clinical research ed.), 342(jun10 1), d3397–d3397. doi:10.1136/bmj.d3397